IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 11 Ver. IV (Nov. 2015), PP 101-105
www.iosrjournals.org
Histopathological Correlation of Lymph Nodes Imprints
Dr. Piyali Kundu1, Dr. Debarati Pathak2, Dr. Seema Mondal3, Dr. Moulik
Debnath4, Dr. Sanchita Saha5, Dr. Tushar Kanti Saha6
1
(Demonstrator, Dept. of Pathology, I.P.G.M.E&R.); {2(Demonstrator) 3(Asst. Prof.) Dept. of Pathology,
Burdwan Medical College & Hospital}; {4(Asst. Prof.) Dept. of Anatomy, 5(Asst. Prof.) Dept. of Medicine}
Murshidabad Medical College & Hospital; 6(Asst. Prof.) Dept. of Community Medicine, North Bengal Medical
College & Hospital6
Abstract:
Introduction: This study was done to evaluate the role of imprint smear cytology in various diseases affecting
the lymph nodes. A correlation was done between the imprint smear cytology and histopathology to assess the
accuracy and reliability of the imprint cytology in different lymph node lesions. Methods: From 52 cases of
lymph node excision, imprint smears were taken and stained with PAP, H & E and MGG. The findings in
imprints were compared with those of histopathology. With the help of sensitivity, specificity & kappa (k) score,
the agreement between the two methods was determined. Results: Among the total 52 cases of imprint smears,
44 cases from breast carcinoma were reactive, among them 8 cases turned positive in histopathological section
but negative in imprint. So, total reactive cases were 36.Out of the cases suspected to be Non-Hodgkins
lymphoma in imprint, 1 small cell lymphoma in imprint was finally diagnosed as mantle cell lymphoma in
histology, & 1 large cell lymphoma in imprint was finally diagnosed as diffuse large B cell lymphoma in
histology, 4 other cases were turned to be reactive in both imprint and HP. Hence the total reactive cases were
40.One (1) metastatic carcinoma from colon & 1 from gallbladder carcinoma were correctly diagnosed by
imprint. Interpretation and Conclusion: Imprint smears showed almost perfect agreement in majority of the
lesions. The technique was simple, rapid and can be used routinely as an adjunct to histopathology of lymph
node lesions.
Keywords: Imprint smear, Lymph node, Non-Hodgkings lymphoma
I. Introduction
The imprint cytology had been in use as a rapid and standard method for diagnosing lymph
adenopathies since several years. Forkner was the first person to utilize imprint technique for cyto-diagnosis in
lesions of excised lymph nodes.
In the later half of the 19th century various studies published on imprint cytology of lymph nodes had
proved it to be an useful adjunct for histopathological diagnosis of inflammatory, granulomatous, lymphomatous
and metastatic lesions of lymph nodes.
II. Materials & Methods
The material for this study was taken from 52 patients in R.G. Kar. Medical College who underwent
lymph nodes excision biopsy. Clinical data collected in each case were: Age and sex, Signs and symptoms, Sites
of lymph nodes involved, associated clinical findings, relevant investigation.
The excised lymph nodes were transported immediately to the laboratory. The gross features of the node were
noted like: Size & Appearance of outer surface.
After describing the gross features, it was sliced into two halves. The sliced half was held gently either
with forceps or with one hand so that the flat cut surface faced upwards; with the other hand, using grease free
clean glass slides, four imprint smears were prepared. The lymph node was then fixed in neutral formalin and
processed for histopathological examination. Wet fixed smears were stained with PAP and H & E. The air dried
smear was stained by MGG stain. Special stains such as AFB stain, reticulin were also done in certain cases.
The stained smears were assessed for the following features:
1. Cellularity: Hypo-cellular - if number of lymphocytes < 50/smear
Moderately cellular - if number of lymphocytes = 50/smear
Hypercellular - if number of lymphocytes > 50/ smear
2. Distribution: Monotonous or Polymorphous
3. Cell Types: Reactive lymphoid cells, Tingible body macrophages, Atypical lymphophoid cells, Granuloma,
Foreign cell.
According to the finding as noted the lesions were classified into a particular type of lesion .The
accuracy of imprint diagnosis was determined by comparing with the corresponding histopathological diagnosis.
DOI: 10.9790/0853-14114101105
www.iosrjournals.org
101 | Page
Histopathological Correlation of Lymph Nodes Imprints
The diagnosis that agreed with the histopathological diagnosis was considered accurate and overall accuracy
rate or sensitivity & specificity was calculated. The sensitivity for each condition of lymph nodes was
calculated. The agreement between the imprint smear diagnosis and histopathological diagnosis was calculated
using kappa score.
III. Results
In our study, out of 52 cases 2 were metastatic and another 2 were lymphoma. Grossly the metastatic
lymph nodes were enlarged in size. Outer surface was grey, cut surface chalky white in colour. The signs and
symptoms of two metastatic diseases were nonspecific, mimicking chronic cholecystitis (pain, anorexia,
elevated alkaline phosphatase). Upper abdominal pain and increased serum alkaline phosphatase level were the
most common findings at presentation in case of gallbladder carcinoma metastatic (Fig 1 &2).12
Colorectal cancer was also asymptomatic for years; symptoms developed insidiously and frequently
had been presented for months, associated with clinical attention by the appearance of fatigue, weakness, and
iron deficiency anemia, occult bleeding, changes in bowel habit, or crampy left lower quadrant discomfort. Both
the cases were associated with enlarged lymph nodes (Fig 3&4).12
Most patients presented with fatigue and lymphadenopathy and were found to have generalized disease
involving the bone marrow, spleen, liver, and (often) the gastrointestinal tract, in mantle cell lymphoma.12
Total case = 52Actual reactive = (44 8) + 4= 36 +4= 40(8 cases in metastatic carcinoma were +ve in
histology but ve in imprint.4 cases suspected of NHL turned to be reactive both in histology & imprint.).
Imprint smears of reactive lymph nodes showed mixed population of cells representing the whole range of
lymphocyte transformation, tingible body macrophages & associated with predominance of small lymphocytes
in cases of reactive lymph nodes.7
Histological section of reactive nodes showed follicles with different size and shape, the margins of
which were sharply defined, surrounded by mantle of small lymphocytes arranged circumferentially as an onion
skin pattern and consisting of admixture of small, large lymphoid cells with irregular nuclei, numerous mitosis
& tingible body macrophages(Fig & 6).8NHL = 2 (Both histology & imprint +ve)
In imprint small cell lymphoma showed pleomorphic small cells with coarse clumped chromatin,
inconspicuous nucleoli, scanty cytoplasm and few prolymphocytes . 7Histology showed lymphoid cells
infiltrated as diffuse, vaguely nodular or nodula pattern where cells proliferated as broad mantles around
residual reactive germinal centres with coalescence and extention into the interfollicular regions. Proliferative
centres were absent butepitheloid histiocytes were seen. 9
Imprint smear of DLBCL showed pleomorphic large cell population dominated by round nuclei,
unevenly distributed nuclear chromatin, prominent usually single central nucleoli, occationally multiple nucleoli
with moderate to abundant bluish cytoplasm.7
Histology of DLBCL showing lymphoid structure had been effaced by diffuse pattern of growth of
large cells, which had round to oval nucleus that appeared vesicular due to margination of chromatin to the
nuclear membrane, but large multilobated or cleaved nuclei Cells had moderately pale or basophilic cytoplasm
and prominent centrally or eccentrally placed nucleoli.10
Metastatic carcinoma = 2 (Both histology & imprint +ve)
Imprint smear of mucinous metastatic colonic adenocarcinoma (Figure-6) showed discohesive three
dimensional aggregates of tumor cells. Branching papillary fragments and microacinar areas might be present in
the pool of mucin. Cell groups showed loss of polarity
with crowded disorderly arrangement.
Tumor cells had round, oval or cigar shaped nuclei, and many single cells. There was a prominent
dirty tumor diathesis.14 Histologically metastatic lymph node of colonic adenocarcinoma showed glands or
irregular cluster of cells which were round to oval in shape, nuclei were uniform retained a basal location and
surrounded by mucus. 9 Imprints of gallbladder adenocarcinoma (Figure - 4) showed loosely structured clusters
of cancer cells with irregular large nuclei and very prominent nucleoli.11 Histologically metastatic lymph node
of gallbladder adenocarcinoma showed the cells which were arranged in nests, sheets, cords or tubular pattern
and had irregular shaped hyperchromatic nuclei, scanty ill defined cytoplasm with inconspicuous nucleoli. 9
IV. Discussion
Imprint smear study was simple, speedy and provided excellent cytomorphological details. The imprint
smears were prepared from 52 freshly excised lymphnodes in ours study, we got 2 NHL and 2 metastatic deposit
out of 52 total cases. There were no cases of Hodgkins disease in the present study. The smears except for few
were adequate when assessed by quality of stain, cellularity and dispersion of cells. 1,2,3
In our study among two cases (4%) : one was small cell lymphoma in imprint which was finally
diagnosed as Mantle zone lymphoma and other large cell lymphoma in imprint was identified as diffuse large B
cell lymphoma. Only two cases were too small for any comments. More number of cases needed to be studied.
DOI: 10.9790/0853-14114101105
www.iosrjournals.org
102 | Page
Histopathological Correlation of Lymph Nodes Imprints
Agarwal et al1, Patra et al 2, Ultman et al 4, Nagpal et al 3 etc. had observed the same type of pathology e. g.
lymphomas.
Agarwal et al1 & Nagpal et al3 observed an incidence 0f 10 to 14 %. The sensitivity in NHL among
workers viz. Agarwal, Patra, Ultman and Nagpal ranged between 3-7%, which was comparable to the present
study though the number of cases was low. Nagpal et al3 found that smears had an even distribution of cells,
with fewer distortions and good coloration of all cellular components providing maximal cytological details.
The examination of smears in such cases revealed uniform results.
Suen et al5 compared imprints and frozen sections of 198 lymph nodes. Their accuracy rate was 93.6%.
They emphasized the usefulness of imprint smears over lesions missed by frozen sections.
Nagpal et al3 also gave the importance of imprint smears compared to that of histopathological sections
and commented that, lymph nodes being cellular organs, were poorly fixed, for which taking of thin sections
became very difficult. Moreover there might be shrinkage of the cells.
In the present study histopathological sections were adequate for comments concerning histological
types. But this investigation was invaluable to diagnose the various categories that could help in the further
management.Of the 10 cases of metastatic lesions in lymph nodes only 2 cases were picked up by imprint
smears. Here the accuracy rate of 2 metastatic deposit was 20%.
In another study by Ultmann et al3 the accuracy for metastatic was found as 94%. They found that
diagnosis of secondaries in a lymph node from tumour else where in the body did not present any diagnostic
problem unless it was a sclerotic lesion. This was also observed in the present study. As the abnormal cancer
cells were invariably present in the smears which were absolutely foreign to the lymphoid elements the
detection did not cause any difficulty3.
Wood WS et al5 commented that hypocellularity and in adequate material were the most probable
cause of false negative diagnosis in imprint. It occurred generally due to one of the following two reasons:
A. Insufficient cells - there was a dense fibrous stroma in some tumors, such as the linitis plastic type
of gastric carcinoma, the breast carcinoma, the gall bladder carcinoma, some fibrous soft tissue tumors etc. In
these cases the number of neoplastic cells transferred to the slide was insufficient to enlable the observer to
make a correct diagnosis.
B. Interpretative errors these occurred in cytological well differentiated tumors.
This present study showed that the detection of cancer cells were difficult in cases where there was
extensive fibrosis, which was discernable in the histopathological sections of the particular lymph nodes. 8 cases
failed to reveal metastatic deposit due to extensive fibrosis in lymph nodes.
Hasenburg et al6, Tatomirovie Zet et all,2,3 reported a sensitivity rate of 90 to 93% and Jain et al 15
reported 100% sensitivity where they had included histopathology along with imprint for such comments. The
present study showed 100% sensitivity when histopathology is included. The fact of extensive fibrosis was
indeed a case of concern when only imprint smears were available for interpretation. The diagnostic sensitivity
was hampered by the fact that small metastatic deposits confined to the sub capsular sinus and single cell
metastatic was missed. However early micro metastases rarely produced significant lymph node enlargement
and a lymph node if palpable was likely to contain enough tumor tissues to be detected. 7 Among the metastatic
lesions seen in our study the incidences were of metastatic mucinous adenocarcinoma of colon & poorly
differentiated adenocarcinoma of gall bladder.
The 52 samples of lymph nodes biopsies included in the study. During the period of study, lymph
nodes were excised after clinical diagnosis of neoplastic lesions. Only 12 cases showed neoplastic changes, the
rest showed reactive changes and thus acted as controls in the study. It was needless to point out that not all
lymph nodes draining malignant lesions would show incidence of metastatic deposits. Many might show only
reactive changes. Provision for these different stains in a country like ours should help in diagnosing the
pathology in quite a few instances.
V. Conclusion
Imprint cytology is a type of applied cytology. The imprint smears reveal very subtle diagnostic
changes in the various lymphoid cells and make it possible to arrive at a diagnosis in shorter period of time.
References
[1]
[2]
[3]
[4]
[5]
Agarwal PK, Gosh M, Wahal KM, Mehrotra RML. Study of imprint smears of lymph nodes. Ind J. of Cancer. 1997; 14 : 157 163.
Patra SP, Bhattacharya N, Mangal S. : FNAC, Imprint cytology and Histopathology for diagnosing diseases of lymph node. Journal
of cytology. 2003; 20 (3) : 124 128.
Nagpal BL, Dhar CN, Singh A, Bahl RA. Evaluation of Imprint Cytodiagnosis in cases of Lymphadenopathy. Indian J. of Pathol
Microbiol. 1982; 25 : 35 39
Ultmann JE, Koprowska I, Engle RL. A cytological study of lymphnode 18imprints Cancer, 1958; 11 : 507-24.
Suen KC, Wood WS, Syed AA, Quenville NF, Clement PB : Role of imprint cytology in intra -operative diagnosis : value and
limitations. Journal of Clinical Pathology. 1978; 31 : 328 337.
DOI: 10.9790/0853-14114101105
www.iosrjournals.org
103 | Page
Histopathological Correlation of Lymph Nodes Imprints
[6]
[7]
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
Hasenburg A, Ledet SC, Ardaman T, Levy T, Kieback DG. Evaluation of lymph nodes in squamous cell carcinoma of the cervix:
touch imprint cytology versus frozen section histology. International Journal of Gynecological Cancer. 1999; 9(4) : 337 341.
Svante R. Orell, Gregory F. Sterrett, Darrei Whitaker. Fine Needle Aspiration Cytology. India: Elsevier; 2010.
Juan Rosai. Rosai And Ackermans Surgical Pathology. China : Mosby Elsevier; 2011.
Christopher D.M. Fletcher. Diagnostic Histopathology Of Tumors. China: Elsevier; 2007.
Vinay Kumar, Abul K. Abbas et al. Robbins and Cotran Pathologic Basis Of Disease. India: Elsevier; 2010.
Das DK. Tripathi RP, Bhambhani S et al. Ultrasound guided fine needle aspiration cytology diagnosis of gallbladder lesions : a
study of 82 cases. Diagn cytopathol 18 : 258- 264, 1998.
N. Volkan Adsay, Geoffrey P. Altshuler et al . Sternbergs Diagnostic Surgical Pathology. China : Wolters Kluwer Health; 2010 .
Feinberg MR., Bhaskar AG., Bourne P. Differential diagnosis of malignant lymphomas by imprint cytology. Acta Cytol. 1980;
24(1) : 16 25.
Mans Akerman, Asmund Berner et al. Diagnostic Cytopathology. China : Elsevier; 2010.
Jain P Kumar R, Anand M, Asthana S, Deo SV, Gupta R et al. Touch imprint cytology of axillary lymph nodes after neoadjuvant
chemotherapy in patients with breast carcinoma.Cancer. 2003; 99 (6) : 346 351
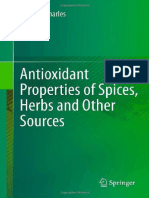
Figure 1: Imprint Smear From Poorly Differentiated
Adeno Carcinoma, Gall Bladder ( MGGX400)
Figure 2: H.P. Section From Poorly Differentiated
Adeno Carcinoma. Gall Bladder (H&E X 400)
Figure 3: Imprint Smear In Metastatic Mucinous
Adeno Carcinoma Colon (MGGX 400)
Figure 4: H.P. Section From Metastatic Mucinous
Adeno Carcinoma Colon (H&E X 400)
DOI: 10.9790/0853-14114101105
www.iosrjournals.org
104 | Page
Histopathological Correlation of Lymph Nodes Imprints
Figure 5: Imprint Smear Of SLL (H & E X 400)
Cervical Lymph Node
Figure 6: H.P. Section Showing Mantel Cell Lymphoma (H&EX400)
DOI: 10.9790/0853-14114101105
www.iosrjournals.org
105 | Page
You might also like
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocument7 pagesSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)No ratings yet
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocument5 pages"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Assessment of The Implementation of Federal Character in Nigeria.Document5 pagesAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)No ratings yet
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocument14 pagesAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)No ratings yet
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Document15 pagesA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)No ratings yet
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocument5 pagesRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)No ratings yet
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocument7 pagesA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)No ratings yet
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)No ratings yet
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocument6 pagesThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)No ratings yet
- The Impact of Technologies On Society: A ReviewDocument5 pagesThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocument7 pagesComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)No ratings yet
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocument4 pagesInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)No ratings yet
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocument6 pagesImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocument5 pagesEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)No ratings yet
- Human Rights and Dalits: Different Strands in The DiscourseDocument5 pagesHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)No ratings yet
- The Lute Against Doping in SportDocument5 pagesThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)No ratings yet
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationDocument3 pagesBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)No ratings yet
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocument7 pagesTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)No ratings yet
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocument6 pagesRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahDocument9 pagesClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)No ratings yet
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsDocument6 pagesAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)No ratings yet
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweDocument9 pagesTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDocument6 pagesKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)No ratings yet
- Women Empowerment Through Open and Distance Learning in ZimbabweDocument8 pagesWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweDocument8 pagesMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextDocument6 pagesDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)No ratings yet
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaDocument11 pagesSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)No ratings yet
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocument5 pagesDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalNo ratings yet
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaDocument3 pagesMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- A Study On The Television Programmes Popularity Among Chennai Urban WomenDocument7 pagesA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Module 22 - EditedDocument26 pagesModule 22 - EditedGabriel Cabansag75% (4)
- Essentials Lab Resource Guide 12 22Document67 pagesEssentials Lab Resource Guide 12 22Aijeleth Shahar Gunay AwacayNo ratings yet
- General Biology 2: Quarter 3: Week 5 and 6 - Module 5 Taxonomy and SystematicsDocument20 pagesGeneral Biology 2: Quarter 3: Week 5 and 6 - Module 5 Taxonomy and Systematicscristina maquinto83% (6)
- The History of GMODocument3 pagesThe History of GMOAnthony JonasNo ratings yet
- USMLE - VirusesDocument120 pagesUSMLE - Virusessapatel89No ratings yet
- Grade 12 Biology Model QuestionsDocument9 pagesGrade 12 Biology Model Questionsmmree yyttNo ratings yet
- Prokaryotes and EukaryotesDocument1 pageProkaryotes and EukaryotesconchoNo ratings yet
- Cholesterol TotalDocument9 pagesCholesterol TotalichaaznNo ratings yet
- HES 087 Microbiology and Parasitology (Instructional Design S.Y. 2020-2021)Document18 pagesHES 087 Microbiology and Parasitology (Instructional Design S.Y. 2020-2021)Ellery L TrumataNo ratings yet
- Course Schedule2016172Document66 pagesCourse Schedule2016172kartavya jainNo ratings yet
- Grade 4 Life Science Structures and FunctionsDocument9 pagesGrade 4 Life Science Structures and Functionszeinab ahmedNo ratings yet
- PLOTKINDocument6 pagesPLOTKINElPaisUyNo ratings yet
- Detection of Inva Gene of Salmonella From Milkfish (Chanos Chanos) at Sidoarjo Wet Fish Market, Indonesia, Using Polymerase Chain Reaction TechniqueDocument7 pagesDetection of Inva Gene of Salmonella From Milkfish (Chanos Chanos) at Sidoarjo Wet Fish Market, Indonesia, Using Polymerase Chain Reaction TechniqueMarsha NajlaNo ratings yet
- Natural History of Eukaryotic DNA Methylation SystemsDocument80 pagesNatural History of Eukaryotic DNA Methylation SystemsDumbo MkuNo ratings yet
- Stas Week 15 GmoDocument2 pagesStas Week 15 GmoZyra PascualNo ratings yet
- A Standardized Terminology For Describing Reproductive Development in FishesDocument20 pagesA Standardized Terminology For Describing Reproductive Development in FishesGisellenLimaNo ratings yet
- GE 7 Module Lesson 3FDocument6 pagesGE 7 Module Lesson 3Faltair sinajonNo ratings yet
- Canal System in Porifera: Ascon, Sycon and Leucon TypesDocument4 pagesCanal System in Porifera: Ascon, Sycon and Leucon TypesZotei RawihteNo ratings yet
- 164-Antioxidant Properties of Spices Herbs and Other Sources Denys J. Charles 1461443091 Springe PDFDocument588 pages164-Antioxidant Properties of Spices Herbs and Other Sources Denys J. Charles 1461443091 Springe PDFmandarim100% (1)
- Preparing A Purification Summary TableDocument6 pagesPreparing A Purification Summary TableAngeles Uribe JiménezNo ratings yet
- Quiz 1 Phylogenetic Trees and Animal BasicsDocument2 pagesQuiz 1 Phylogenetic Trees and Animal Basicsapi-413777206No ratings yet
- Animal Diversity NOTE - 111104Document5 pagesAnimal Diversity NOTE - 111104Mohammed KasimNo ratings yet
- Villaseñor & Espinosa. 2004. Alien Flowering Plants in MéxicoDocument11 pagesVillaseñor & Espinosa. 2004. Alien Flowering Plants in MéxicopolleiriNo ratings yet
- Byjus Com Biology Plant PhysiologyDocument14 pagesByjus Com Biology Plant PhysiologyVikas PratikNo ratings yet
- Worksheet in Mitosis and MeiosisDocument5 pagesWorksheet in Mitosis and MeiosisJudarlyn Madria0% (1)
- Sbi3ui DR EvolutionDocument3 pagesSbi3ui DR Evolutionapi-234678275No ratings yet
- Evolution of Social BehaviorDocument48 pagesEvolution of Social BehaviorNaniNo ratings yet
- Takahashi 1991Document7 pagesTakahashi 1991Tibor SzénásiNo ratings yet
- Lecture 5 - Enzymes and CoenzymesDocument7 pagesLecture 5 - Enzymes and CoenzymesDoreenNo ratings yet