Journal of Gerontology: BIOLOGICAL SCIENCES
1998, Vol. 53A, No. 4, B274-B280
Copyright 1998 by The Gerontological Society of America
Age-Related Changes of Arterial Mechanical
Properties in Rats: Analysis Using Exponentially
Tapered T-Tube Model
Kuo-Chu Chang, Yuan-Feen Tsai, Chai-Yee Chow, Ying-I Peng, and Tong-J Chen
Department of Physiology, College of Medicine, National Taiwan University, Taipei, Taiwan.
T has been suggested that arterial physical properties,
such as elasticity and distensibility, change with age
(1-4). Histological alterations of the vasculature, including
the degeneration of smooth muscles in the media, the fragmentation and decrease of elastic fibers, and increases of
irregularly arranged collagen fibers in the stroma, become
obvious in elderly populations (5). In humans, the changes
of the mechanical properties occur primarily in large vessels. The stress-strain data of blood vessels show an increase in the elastic modulus or a decrease in the distensibility of aged human vasculature (6-8). The changes in
aging dog seem to be similar to those in human (9,10).
However, the age-related changes in the rabbit are opposite
to those reported in human (11). Contradictory observations were reported in rats, showing no change (12), an
increase (13), or a decrease (14) in the elastic modulus with
age. These data seem to suggest that the variance may be
caused by the difference in species or analytical methods.
Because the mechanical properties of the vasculature can
be reflected in the aortic pressure-flow relation, measurements of the aortic input impedance are regarded as essential for the analysis of the arterial mechanics (15-18). Both
model-independent and model-based approaches have been
adopted to obtain the aortic input impedance. The modelindependent approach, such as Fourier series expansion of
the aortic pressure and flow signals, involves direct
description of the arterial mechanics (15,16). This approach
tends to be purely observational and may overlook the
complexity of the distributed vasculature. The model-based
approach, such as wave transmission model based on Ttube topology, has been used to explain the arterial wave
B274
propagation and reflection phenomena (19,20). However,
in the mammalian arterial system, the nature of the vasculature is nonuniformity (16,18,21). In earlier analysis, the
changes of vascular diameter and elastic tapering have not
been taken into consideration. A new approach with the
exponentially tapered T-tube model was developed recently
to relate the pulsatile pressure and flow waves measured in
the ascending aorta (22). The method can reflect the physiological behavior of arterial diameter and elastic tapering
and is considered as a proper mean to analyze aortic input
impedance. The analysis will provide insightful information of the wave transmission in the arterial system.
Earlier studies on the changes of vascular physical properties to rats showed great diversity in response to age.
Therefore, the purpose of this study was to reexamine the
changes of rat's arterial mechanical properties in relation to
age by using the exponentially tapered T-tube model. The
aortic characteristic impedance, arterial load compliance,
vascular tapering index, and amplitude as well as timing
of pulse wave reflection were analyzed to delineate the
changes in arterial mechanical properties.
MATERIALS AND METHODS
Subjects
The specific pathogen-free male Long-Evans rats used in
this study were obtained from the colony maintained in the
barrier facilities at the Animal Center of Medical College,
National Taiwan University. All rats were allowed free
access to the Purina chow and water and housed two to
three per cage in a 12-h light/dark cycle animal room. Peri-
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
This study was designed to explore the changes of mechanical properties in the rat's arterial system at different ages
by using the exponentially tapered T-tube model. Long-Evans male rats at the ages of 6, 12, and 18 months were
anesthetized and thoractomized. Rats at the ages of 6, 12, and 18 months were individually referred to as young,
adult, and middle-aged rats. The pulsatile pressure and flow signals in the ascending aorta were measured by a
high-fidelity pressure sensor and electromagnetic flow probe, respectively. Model parameters, such as aortic characteristic impedance, vascular tapering index, wave transit time, and arterial load compliance, were inferred from the
aortic pressure and flow signals to describe the pulsatile nature of blood flows in the vasculature. The static hemodynamic condition in those animals with different ages was characterized by (i) no change in cardiac output and (ii)
a decrease in heart rate, arterial blood pressure, as well as total peripheral resistance. As for the pulsatile nature of
the arterial system, the wave transit time remained unaltered, indicating there was no change in the aorta's distensibility of rats at those three different ages. The arterial load compliance, which describes the buffering nature of a
hollow vessel, also remained unchanged. On the contrary, there was a significant fall in aortic characteristic
impedance in those age-related rats. The decline of aortic characteristic impedance without a significant change in
arterial distensibility suggests that lumen growth of the aorta and large arteries may occur in rats up to middle age.
VASCULAR DYNAMIC CHANGES IN AGE-RELATED RATS
odic checks of the cages and body weights ensured that the
food was administered properly. Rats at the ages of 6 (n =
10), 12 (n = 10), and 18 months (n = 10) were anesthetized
and thoractomized for the study of age-related changes in
arterial mechanical properties. Rats at the ages of 6, 12, and
18 months were referred to as young, adult, and middleaged rats, respectively.
Model Parameters Inferred by the Exponentially Tapered
T-Tube Model
All model parameters were estimated and analyzed by
the exponentially tapered T-tube model according to the
procedure described previously (22). In brief, an asymmetric T-tube model with vascular nonuniformity was used to
relate the pulsatile pressure and flow waves in the ascending aorta. The nonuniform T-tube model and its terminal
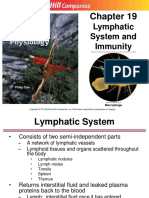
complex load are shown in Figure 1. This model consists of
two sections of different lengths. The shorter section represents the circulation of head, neck, and upper limbs (head
or upper body circulation), and the longer section represents the circulation of trunk and lower limbs (body or
lower body circulation). The subscripts h and b represent
the head and body circulation, respectively. Properties of
the ith tube, / equals h or b, include a characteristic impedance (Zci) at the entrance of the tube and a transmission
time (T,). T, is the time for a wave to propagate from one
end of the tube to the other. Properties of the load are given
by the load elements that are high-frequency tube-matching
impedance element (/?,), load compliance (Cu), and terminal resistance (/?,) The relation between the characteristic
impedance at the distal end of the tube and that at the
entrance of the tube is quantified by the tapering index
(^^oOw-^oo (22). In this system, the parallel combination of
the head circulation and body circulation is defined as the
global circulation. Peripheral resistance of the global circulation (Rp) was calculated as mean pressure divided by
mean flow. The terminal resistance of each tube was computed by using the upper-to-lower body resistance ratio of
2.33 for normotensive state and 3.17 for hypotensive state
(see Appendix, Note 1). With setting (^Go^o)-^ equal to
(#I.6O<,)<D->OO, the model parameters, such as aortic characteristic impedance (Zc), vascular tapering index (qQ0)oi^,
wave transit time (T^T*), and arterial load compliance
(Cu,,Cu,), were estimated by using the equations developed
for the exponentially tapered T-tube model. The characteristic impedance at the inlet of each tube was calculated by
using the upper-to-lower body characteristic impedance
ratio of 1.14 for normotensive condition and 1.20 for
hypotensive condition (see Appendix, Note 2). The high-frequency tube-matching impedance was determined by the
characteristic impedance, tapering index, and terminal resistance (22). The time domain reflection factor was derived as
the amplitude ratio of backward-to-forward peak pressure
wave according to previously described methods (27).
Therefore, the wave reflection phenomenon was characterized by the wave transit time and the wave reflection factor.
In the process of model parameter estimation, the measured aortic pressure was taken as the output variable
whereas the measured aortic flow was the model input variable. Parameters of the model were adjusted to minimize
the normalized root-mean-square error (e*), using the
Nelder-Meade Simplex algorithm (28). The model parameters leading to the minimum of e* were taken as the model
estimates of arterial mechanical properties. In one rat,
examples of the measured (solid lines) flow wave and pulsatile pressure in the ascending aorta and the mathematically predicted (dashed lines) results were shown in the top
of Figure 2. The input impedance spectra of the same rat
were shown in the bottom of Figure 2. The solid lines represented the model-generated spectra, and the circles were
data points obtained from the ratio of the ascending aortic
pressure harmonics to the corresponding flow harmonics.
The aortic impedance spectra of the measured and mathematically deduced results were similar.
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
Catheterization
Each rat was anesthetized with sodium pentobarbital (35
mg/kg, i.p.). The femoral vein was cannulated for the
administration of supplemental pentobarbital (30 mg/kg
every 2 h). Tracheotomy was performed to provide artificial
ventilation with a tidal volume of 6-8 ml/kg and respiratory
rate of 50-70 breaths/min (23,24). The chest was opened
through the right second intercostal space. An electromagnetic flow probe (model 100 series, internal circumference 8
mm, Carolina Medical Electronics, King, NC) was placed
around the ascending aorta to measure the pulsatile aortic
flow. A Millar catheter with a high-fidelity pressure sensor
(model SPC 320, size 2F, Millar Instruments, Houston, TX)
was used to measure pulsatile aortic pressure. Before inserting the catheter, the pressure sensor was prewarmed in 37C
saline for at least 1 h. The catheter was inserted via the isolated right carotid artery into the ascending aorta. The
catheter tip position of the pressure transducer was adjusted
1-2 mm distal to the downstream edge of the electromagnetic flow probe to avoid interference with the flow measurements. After withdrawing the catheter from each rat, the
catheter was reimmersed in the bath to check for baseline
drift. At the end of the experiment, the pressure reading
from the sensor barely submerged in the saline at atmospheric pressure and room temperature was used as the zero
pressure reference (25). Timing between the pulsatile pressure and flow signals, due to spatial distance between the
flow probe and proximal aortic pressure transducer, was corrected by a time-domain approach, in which the foot of the
pressure waveform was realigned with that of the flow (26).
The electrocardiogram (ECG) of lead II was recorded with a
Gould (Cleveland, OH) ECG/Biotach amplifier. The analogue waveforms were sampled at 500 Hz by using a 12-bit
simultaneously sampling analog-to-digital (A/D) converter
interfaced to a personal computer. Selection of signals (5-10
beats at steady state) was made on the basis of the following
criteria: (i) recorded beats with optimal velocity profile that
was characterized by a steady diastolic level, maximal systolic amplitude, and minimal late systolic negative flow; (ii)
beats with an RR interval, cardiac cycle length, less than 5%
different from the average value for all recorded beats; and
(iii) exclusion of ectopic and postectopic beats. The selective beats were averaged in the time domain, using the peak
R wave, the peak wave of QRS, of ECG as a fiducial point
and were subjected for further analysis.
B275
CHANG ETAL.
B276
Head End
Complex Load
'ch
Complex Load
Complex Load
Body End
Figure 1. T-tube arterial system model with asymmetric head and body circulation paths. Each path consists of a nonuniform lossless transmission tube
and a complex terminal load. Properties of each tube include an input characteristic impedance Z and a characteristic delay time Ti for wave transmission
from one end of the tube to the other. The quantity exp((^0o)a)-+oo) is used to relate the characteristic impedance at the distal end of the tube to that at the
inlet of the tube. Complex loads possess /?,, Cu, and Rpi as described in the text [from Chang and Kuo (22)].
Fitness of the data generated by the model was judged by
the magnitude of e* and by indices from a linear regression
of the model-generated pressure on the measured pressure.
Two indices were used to evaluate the goodness-of-fit: (i) the
coefficient of determination r\ and (ii) the standard error of
the estimate SEE. We looked for r2 to be close to 1 and for
SEE to be of order of 1% when expressed relative to the
mean of all pressure observations. A summary of the measures indicating goodness of the exponentially tapered T-tube
model fits was given in Table 1. Sensitivity analysis on the
model parameters was also performed to give insight into
these estimators (29). The relative standard error of the
parameters over all experimental rats were as follows: 5.4
1.4% for T, 3.8 1.6% for T, 5.2 1.9% for Cu,, 5.2 1.5%
for Cu,, 1.8 0.7% for Zc, and 6.4 2 . 1 % for (g0o)a>->oo.
These results indicated that all model parameters were estimated with good accuracy in analyzing the systemic arterial
system with the exponentially tapered T-tube model.
Statistics
Results were expressed as means SE. When multiple
comparisons were made for the age effect on the arterial
mechanical properties, statistical significance was determined by analysis of variance (ANOVA). Significant differ-
ences were assumed at the level of/? < .05. If ANOVA for a
hemodynamic variable reached the significant level, then
the Tukey method was used to determine the groups of rats
having different mean values of the variable.
RESULTS
The effect of age on body weight, heart rate, arterial
blood pressure, and cardiac output was shown in Table 2.
Body weight was similar between 12- and 18-month-old
rats and was significantly smaller in 6-month-old rats. A
significant decrease in heart rate, systolic, diastolic, and
mean arterial blood pressure was observed in 18-month-old
rats relative to 12-month-old rats. Cardiac output was not
changed in rats at the ages of 6, 12, and 18 months. However, total peripheral resistance was significantly decreased
in 18-month-old rats.
Table 3 lists the global vascular parameters that were
estimated by the exponentially tapered T-tube model. Rats
at 18 months old had a significant fall in aortic characteristic impedance, whereas rats between 6 and 12 months old
had no significant change in this parameter. Vascular tapering index, wave reflection factor, and total load compliance
were similar among rats at the ages of 6, 12, and L8
months. The pulsatile nature of blood flows in each tube
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
PC)
B277
VASCULAR DYNAMIC CHANGES IN AGE-RELATED RATS
100
150
200
Time (msec)
20
50
100
150
200
Time (msec)
40
60
Frequency (Hz)
20
Frequency (Hz)
Figure 2. Example of pulsatile waves and aortic input impedance in one rat. (Top) Pressure and flow signals measured in the ascending aorta (solid
lines); pressure predicted by the exponentially tapered T-tube model (dashed line). (Bottom) Input impedance spectra of head circulation (dashed lines),
body circulation (dotted lines), and global circulation (solid lines), as represented by the exponentially tapered T-tube model. Data points obtained from
the ratio of ascending aortic pressure harmonics to the corresponding flow harmonics (circles).
Table 1. Indexes of Fitness for the Exponentially Tapered T-Tube
Model-Derived Data to 6-, 12-, and 18-Month-Old Rats
Age (month)
Rats
Normalized root-meansquare error (e*) (X10 J )
Standard error of the
estimate (%)
6(n=10)
12 (n = 10)
18 (/i = 10)
6.16 .49
5.86 .57
6.19 .28
.91 .24
.95 .22
.99 .17
Coefficient of determination .9902 .0017 .9899 .0016 .9896 .0014
Notes: All values are expressed as means SE. These indexes are the
linear regression parameters of the model output pressure over the measured pressure.
and terminal load, represented by wave transit time and
arterial load compliance, respectively, were inferred by the
exponentially tapered T-tube model; they are summarized
in Table 4. There was no significant change in wave transit
time in the head and body circulation among rats at those
three different ages. Similar was the arterial load compliance in the head and body circulation of those three groups
of rats. From Tables 2-4 we drew the results that no significant changes were found in the static and oscillatory components of the ventricular afterload inposed on the heart,
when comparison was made only on rats between 6 and 12
months old. These data suggest that the functions of Winkessel and resistance vessels were not modified between
rats at the ages of 6 and 12 months.
We also performed a power analysis to discuss the size of
the difference that would be theoretically important and to
indicate what size of difference could actually be detected
with 80% power. We took CL as an example to delineate
this idea. For CL there was a complete nonsignificant age
difference. Because its standard deviation was about .65,
we could detect a difference on the order of 2.56, 3.00, and
3.54 across the ages with 80% power. A change any smaller
than this would not be of much theoretical importance, so
we feel that this result shows that there is no important age
change in this variable. For Zc it exhibited changes with
age, but not significantly between 6- and 12-month-old animals. The power analysis pointed out that the smallest true
mean difference was about .42 with 80% probability using
the F test between 6- and 12-month-old rats. The analysis
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
50
B278
CHANG ETAL.
Table 2. Basic Hemodynamic Data Measured and Calculated in 6-, 12-, and 18-Month-Old Rats
Age (month)
p- Value
Rats
6 (n = 10)
12 (n = 10)
18 (n = 10)
ANOVA
6vs 12
6vs 18
12 vs 18
BW
HR
P,
419.9 11.1
351.47.13
125.5 2.9
87.9 2.4
106.5 2.4
1.48 .11
75.6 5.9
503.0 15.3
346.7 8.6
127.2 2.6
93.7 3.4
110.7 3.0
1.50.ll
77.7 6.1
508.2 17.1
312.6 12.1
115.8 1.8
83.6 2.1
100.8 2.1
1.76 .07
58.2 2.9
<.001
<.O1
<.O1
<.O5
<.O5
NS
<.O5
<.O1
NS
NS
NS
NS
NS
NS
<.O1
<.O5
<.O5
NS
NS
NS
= .06
NS
<.O5
<.O1
<.O5
<.O5
NS
<.O5
Pi
Pm
CO
Rf
Table 3. Global Parameters Inferred by the Exponentially Tapered T-Tube Model in 6-, 12-, and 18-Month-Old Rats
Age (month)
Rats
Z
R;
p- Value
6 ( = 10)
12 (n = 10)
18(n=10)
ANOVA
6vs 12
6vs 18
12 vs 18
3.09 .20
.1967 .013
.40 .04
2.56 .24
2.87 .19
.1939 .015
.43 .04
2.67 .19
2.10 .14
.1866 .009
.54 .06
2.72 .19
<.005
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
<.05
NS
NS
NS
Notes: All values are expressed as means SE. Zc, aortic characteristic impedance (mmHgmin/ml); (qQo)(ji-*, tapering index; /?/, wave reflection factor, CL, peripheral load compliance (ul/mmHg); NS, not significant (p > .05).
Table 4. Peripheral Load Compliance and Wave Transit Time of the Head and Body Circulation Estimated
by the Exponentially Tapered T-Tube Model in 6-, 12-, and 18-Month-Old Rats
Age (month)
Rats
6 (n = 10)
12 (n= 10)
p- Value
18(n=10)
ANOVA
6vs 12
6vs 18
12 vs 18
Head circulation
Peripheral load
Cu,
.48 .07
.49 .06
.43 .03
NS
NS
NS
NS
3.85 .64
4.50 .93
5.24 .62
NS
NS
NS
NS
Transmission tube
Body circulation
Peripheral load
Cu,
2.08 .23
2.18 .17
2.29 .20
NS
NS
NS
NS
26.69 .98
24.79 .68
25.29 .88
NS
NS
NS
NS
Transmission tube
Tj,
Notes: All values are expressed as means SE. Cu, and Cu,, peripheral load compliance in the head and body circulation, respectively (ul/mmHg);
T and T, wave transit time in the head and body circulation respectively (ms); NS, not significant (p > .05).
reported that if there was a true mean drop of .42 in Zc then
the study has a good chance of detecting it. If the true mean
change were smaller, the study could more easily miss it.
DISCUSSION
This is the first report of using the exponentially tapered
T-tube model to analyze the changes of arterial physical
properties in rats at the ages of 6, 12, and 18 months. The
impedance is determined by the physical characteristics of
the vasculature, including its elastic properties and size, as
well as by the viscosity and density of the fluid contained
within (15,16). Both model-independent and model-based
approaches have been adopted to study aortic input impedance. Because of the arterial distribution, a model-based
approach, such as a succinct T-tube model, is more approapriate for the exploration of the pulsatile nature of blood
flows in the vasculature. Because the diameter and elastic
tapering are of importance in the arterial system (16,18,21),
the smooth change of vascular impedance, caused by these
tapers, must have substantial impact on the magnitude
and/or timing of pulse wave reflection. The diameter and
elastic tapering of the vasculature were taken into consideration in the present study to analyze the changes of vascular
dynamics in rats at those three different ages.
The static hemodynamic condition in rats at the ages of
6, 12, and 18 months was characterized by (i) no change in
cardiac output and (ii) a decline in heart rate, systolic, diastolic, as well as mean arterial blood pressure. There was a
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
Notes: All values are expressed as means SE. BW, body weight (g); HR, heart rate (beats/min); P,, systolic pressure (mmHg); Pd, diastolic pressure
(mmHg); Pm, mean pressure (mmHg); CO, cardiac output (ml/min); Rp, total peripheral resistance (mmHg*min/ml); NS, not significant {p > .05).
VASCULAR DYNAMIC CHANGES IN AGE-RELATED RATS
Just as the elastic modulus is an expression employed to
characterize material properties, so distensibility is a term
used to describe the elastic behavior of a hollow vessel or
chamber. However, compliance and distensibility are quite
different, for compliance is equal to distensibility times
volume (33). In the present study, there were no significant
changes in arterial load compliance among rats at the ages
of 6, 12, and 18 months. No significant changes in arterial
compliance and distensibility suggest that arterial blood
volume may remain unaltered in rats at those three different
ages. However, there were few data in the literature to
describe the blood volume in systemic arterial trees in rats.
Further studies on the changes of arterial blood volume in
age-related rats are needed to delineate the age effect on
homeostasis of the body fluid.
Some limitations of the current study deserve consideration. In this report, the results pertained only to measurements made in the open-chest rat with anesthesia. This setting induced a fall in blood pressure and may introduce
reflex effects not found in the close-chested setting (25). Just
how much anesthesia and thoractomy affect pulsatile hemodynamics in rats was uncertain. However, studies on other
animal models suggest that the effects are small relative to
biological and experimental variability between animals (9).
The major conclusions arising from this study are as follows: (i) Up to middle age in rats, there is a significant fall
in heart rate, arterial blood pressure, total peripheral resistance, and aortic characteristic impedance; (ii) The ageassociated increase in arteriolar caliber in rats may be the
factor responsible for the decrease of total peripheral resistance and therefore the decrease of mean arterial blood pressure; (iii) The decline of aortic characteristic impedance
without significant change in wave transit time suggests that
lumen growth of the aorta and large arteries may occur in
rats up to the middle age.
ACKNOWLEDGMENTS
This study was supported by grants from the National Science Council
(NSC 86-2314-B-002-093-M04). We greatly thank Miss Mei-Yun Tai for
the experimental preparation of this study.
Address correspondence to Dr. Kuo-Chu Chang, Department of Physiology, College of Medicine, National Taiwan University, No. 1, Sec. 1,
Jen-Ai Rd., Taipei, Taiwan.
REFERENCES
1. Lakatta EG. Alterations in the cardiovascular system that occur in
advanced age. Fed Proc. 1979;38:163-167.
2. Lakatta EG, Yin FCP. Myocardial aging: functional alterations and
related cellular mechanisms. Am J Physiol. 1982;242:H927-H941.
3. Newman DL, Lallemand RC. The effect of age on the distensibility of
the abdominal aorta of man. Surg Cynecol Obstet. 1978,147:211214.
4. Yin FCP. The aging vasculature and its effects on the heart. In: Weisfeldt ML, ed. The Heart in Old Age: Its Function and Response to
Stress. New York: Raven; 1980:137-217.
5. Toda T, Tsuda N, Nishimori I. Morphometrical analysis of the aging
process in human arteries and aorta. Ada Anat. 1980; 106:35-44.
6. Learoyd BM, Taylor MG. Alterations with age in the viscoelastic
properties of human arterial walls. Ore Res. 1966; 18:278-292.
7. Mirsky I, Janz RF. The effect of age on the wall stiffness of the
human thoracic aorta: a large deformation anisotropic elastic analysis.
JTheorBiol. 1976;59:467-484.
8. Roach M, Burton AC. The effect of age on the elasticity of the human
iliac arteries. Can J Biochem Physiol. 1959;37:557-570.
9. Cox RH. Three-dimensional mechanics of arterial segments in vitro
methods. JAppl Physiol. 1974;36:381-384.
10. Tanaka T, Fung YC. Elastic and inelastic properties of the canine
aorta and their variation along the aortic tree. J Biomech. 1974;7:
357-370.
11. Saxton JA. Elastic properties of the rabbit aorta in relation to age.
ArchPathol. 1942;34:262-274.
12. Berry CL, Greenwald SE, Rivett JF. Static mechanical properties of
the developing and mature rat aorta. Cardiovas Res. 1975;9:669678.
13. Cox RH. Effects of age on the mechanical properties of rat carotid
artery. Am J Physiol. 1977;233:H256-H263.
14. Hume JF. The tensility of the rat's aorta as influenced by age, envi-
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
report that cardiac output is unaffected by age in rats up to
18 months old (30). The decline in heart rate was described
in rats with advancing age (31,32). Although the effect of
age on arterial blood pressure has been inconclusive, a
recent study has noted that arterial blood pressure decreases
with age in rats (31). Our results of age-related changes in
cardiac output, heart rate, and arterial blood pressure were
in accordance with these reports.
A significant fall in total peripheral resistance was observed in 18-month-old rats. Hydraulic vascular resistance,
a parameter defined as the ratio of driving pressure to flow,
is directly proportional to the viscosity of the blood and
inversely proportional to the fourth power of the tube radius
(15,16). Because there was no evidence of diseases affecting
the viscosity of the blood, the decline in total peripheral
resistance suggests that an increase in arteriolar caliber
occurred in 18-month-old rats. The maintenance of blood
flows for the metabolic needs of bodily organs and tissues
indicated that the decrease in total peripheral resistance may
be the factor responsible for the decline of arterial blood
pressure in middle-aged rats. The decrease in arterial blood
pressure in the absence of significant change in cardiac output may contribute to a smaller steady fraction of total ventricular external power in 18-month-old rats.
In a hydraulic vascular system, the ratio of pulsatile pressure to flow is termed the characteristic impedance if only
centrifugal waves are present at the origin (16). Characteristic impedance is directly related to the blood density and
pulse wave velocity and is inversely related to the lumen
radius squared of the tube. For large arteries, pulse wave
velocity may be approximately related to the elastic modulus of the vessel: the stiffer the vessel, the higher the pulse
wave velocity. Thus, the net result of age on aortic characteristic impedance would be dependent on the relative influence of these counter-balancing factors.
Rats aged 18 months had a significant fall in aortic characteristic impedance. Similarly, Cox (13) calculated the characteristic impedance in rat carotid arteries and found that the
characteristic impedance was actually lower in aging rats. As
for arterial distensibility, Berry et al. (12) showed no change
in the elastic modulus with age in rats. In the present study,
the wave transit time in the head and body circulation, which
is inversely determined by the pulse wave velocity, remained
unchanged in 18-month-old rats. No significant change in
wave transit time reflected that the aorta and large arteries in
18-month-old rats were as distensible as those in 6- and 12month-old rats. The decline of aortic characteristic impedance without significant change in arterial distensibility
suggests that lumen growth of the aorta and large arteries
occurred in rats up to the middle age.
B279
B280
15.
16.
17.
18.
19.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
ronmental temperature, and certain toxic substances. Am J Hyg Sci.
1939;29:ll-23.
McDonald DA. Blood Flow in Arteries. London, UK: Arnold; 1974.
Milnor WR. Hemodynamics. Baltimore, MD: Williams & Wilkins;
1989.
O'Rourke MR Vascular impedance in studies of arterial and cardiac
function. Physiol Rev. 1982;62:571-652.
Taylor MG. Wave travel in arteries and the design of the cardiovascular system. In: Attinger EO, ed. Pulsatile Blood Flow. New York:
McGraw-Hill; 1964:343-372.
Berger DS, Li JKJ, Noordergraaf A. Differential effects of wave
reflection and peripheral resistance on aortic blood pressure: a modelbased study. Am J Physiol. 1994;266:H1626-H1642.
Burattini R, Campbell KB. Modified asymmetric T-tube model to
infer arterial wave reflection at the aortic root. IEEE Trans Biomed
Eng. 1989:36:805-814.
Chang KC. Reply to professor Burattini's comments on "exponentially tapered T-tube model of systemic arterial system in dogs." Med
EngPhys. 1996; 18:336-338.
Chang KC, Kuo TS. Exponentially tapered T-tube model in characterizing arterial nonuniformity. J TheorBiol. 1996; 183:35-46.
Cilley RE, Wang JY, Coran AG. Lung injury produced by moderate
lung overinflation in rats. J Pediat Surg. 1993;28:488-495.
Zhou KR, Lai YL. Capsaicin pretreatment attenuates monocrotalineinduced ventilatory dysfunction and pulmonary hypertension. J Appl
Physiol. 1993:75:2781-2788.
Zuckerman BD, Yin FCR Aortic impedance and compliance in hypertensive rats. Am J Physiol. 1989;257:H553-H562.
Mitchell GF, Pfeffer MA, Westerhof N, Pfeffer JM. Measurement of
aortic input impedance in rats. Am J Physiol. 1994;267:H1907-H1915.
Westerhof N, Sipkema P, Vanden Bos GC, Elzinga G. Forward and
backward waves in the arterial system. Cardiovasc Res. 1972;6:
648-656.
Dennis J, Woods DJ. New computing environments. In: Wouk A, ed.
Microcomputers in Large-Scale Computing. Philadelphia, PA: SIAM;
1987:116-122.
Bard Y. Nonlinear Parameter Estimation. New York: Academic; 1974.
Starnes JW, Rumsey WL. Cardiac energetics and performance of
exercised and food-restricted rats during aging. Am J Physiol. 1988;
254:H599-H608.
Bunag RD, Krizsan D, Eriksson L. Mediation of reflex tachycardia
becomes exclusively 3-adrenergic in old Fischer 344 rats. Mech Ageing Dev. 1990:52:179-194.
Bunag RD, Teravainen TL. Waning cardiovascular responses to
adrenergic drugs in conscious ageing rats. Mech Ageing Dev. 1991;61:
313-326.
Guyton AC. Textbook of Medical Physiology. Philadelphia, PA: W. B.
Saunders; 1991.
Kuwahira I, Heisler N, Piiper J, Gonzalez NC. Effect of chronic
hypoxia on hemodynamics, organ blood flow and O2 supply in rats.
Respir Physiol. 1993;92:227-238.
35. Campbell KB, Burattini R, Bell DL, Kirkpatrick RD, Knowlen GG.
Time-domain formulation of asymmetric T-tube model of arterial system. Am J Physiol. 1990;258:H1761-H1774.
Received April 1, 1997
Accepted February 11, 1998
Appendix
Note 1
The upper-to-lower body resistance ratio can be determined
when the ratio Kaa between measured descending thoracic aorta
mean flow and cardiac output is calculated (20). Under basal condition, approximately 67% of cardiac output in rats consisted of
blood flows in kidneys, spleen, small and large intestines, liver,
stomach, diaphragm, hindlimb muscles and bones, and skin (34).
If blood flow of other tissue and organ in the lower portion of the
body was included, it was speculated that Kd,a in the rat would be
similar to that in the dog [70% in Campbell's report (35)]. From a
comparative physiological point of view, the ratio of Kd,a in rats
was then assumed to be 0.7, .62, and .76 as in dogs under basal,
vasoconstricted, and vasodilated conditions, respectively (35).
Being calculated by the equation of RPJRPb = KdJ(\-Kdla), the
upper-to-lower body resistance ratio was 2.33 for normotensive
state and 3.17 for hypotensive state.
Note 2
The aortic characteristic impedance Zc can be measured by
many different methods. One method is to calculate Zc by averaging high-frequency moduli of impedance data points obtained from
the ratio of the corresponding harmonics of pressure and flow.
From knowledge of Zc, the ratio of upper-to-lower body characteristic impedance Ku, could be inferred by the exponentially tapered
T-tube model. In that case, the ratio of upper-to-lower body characteristic impedance rather than the aortic characteristic impedance
remained to be estimated. With 10 rats, we have separately determined Khb for basal, vasoconstricted (0.5 mg/kg methoxamine, n =
5), and vasodilated (0.5 mg/kg prazosin, n = 5) conditions. The
ratio of upper-to-lower body characteristic impedance was estimated to be 1.142 .083, 1.375 .105, and 1.203 .088 for basal,
vasoconstricted, and vasodilated states, respectively.
Downloaded from http://biomedgerontology.oxfordjournals.org/ at National Taiwan Univ. Hospital on November 23, 2011
20.
CHANG ETAL.
You might also like
- tmp3CAB TMPDocument16 pagestmp3CAB TMPFrontiersNo ratings yet
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersNo ratings yet
- tmpCE8C TMPDocument19 pagestmpCE8C TMPFrontiersNo ratings yet
- tmp80F6 TMPDocument24 pagestmp80F6 TMPFrontiersNo ratings yet
- tmpF178 TMPDocument15 pagestmpF178 TMPFrontiersNo ratings yet
- tmpFFE0 TMPDocument6 pagestmpFFE0 TMPFrontiersNo ratings yet
- tmpEFCC TMPDocument6 pagestmpEFCC TMPFrontiersNo ratings yet
- tmp6F0E TMPDocument12 pagestmp6F0E TMPFrontiersNo ratings yet
- tmpF407 TMPDocument17 pagestmpF407 TMPFrontiersNo ratings yet
- tmpE7E9 TMPDocument14 pagestmpE7E9 TMPFrontiersNo ratings yet
- tmpF3B5 TMPDocument15 pagestmpF3B5 TMPFrontiersNo ratings yet
- Tmpa077 TMPDocument15 pagesTmpa077 TMPFrontiersNo ratings yet
- tmp72FE TMPDocument8 pagestmp72FE TMPFrontiersNo ratings yet
- tmpE3C0 TMPDocument17 pagestmpE3C0 TMPFrontiersNo ratings yet
- tmp998 TMPDocument9 pagestmp998 TMPFrontiersNo ratings yet
- tmp4B57 TMPDocument9 pagestmp4B57 TMPFrontiersNo ratings yet
- tmpC0A TMPDocument9 pagestmpC0A TMPFrontiersNo ratings yet
- tmp6382 TMPDocument8 pagestmp6382 TMPFrontiersNo ratings yet
- tmp60EF TMPDocument20 pagestmp60EF TMPFrontiersNo ratings yet
- tmp8B94 TMPDocument9 pagestmp8B94 TMPFrontiersNo ratings yet
- tmp9D75 TMPDocument9 pagestmp9D75 TMPFrontiersNo ratings yet
- tmp37B8 TMPDocument9 pagestmp37B8 TMPFrontiersNo ratings yet
- tmpD1FE TMPDocument6 pagestmpD1FE TMPFrontiersNo ratings yet
- tmpB1BE TMPDocument9 pagestmpB1BE TMPFrontiersNo ratings yet
- tmp27C1 TMPDocument5 pagestmp27C1 TMPFrontiersNo ratings yet
- tmpA0D TMPDocument9 pagestmpA0D TMPFrontiersNo ratings yet
- tmpC30A TMPDocument10 pagestmpC30A TMPFrontiersNo ratings yet
- Tmp75a7 TMPDocument8 pagesTmp75a7 TMPFrontiersNo ratings yet
- tmp2F3F TMPDocument10 pagestmp2F3F TMPFrontiersNo ratings yet
- tmp3656 TMPDocument14 pagestmp3656 TMPFrontiersNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Presentation of DiptheriaDocument45 pagesPresentation of DiptheriaR-o-N-n-e-lNo ratings yet
- Developmental Biology QuestionsDocument10 pagesDevelopmental Biology QuestionsSurajit Bhattacharjee100% (1)
- Nervous System Lab ReportDocument10 pagesNervous System Lab Reportapi-269985211No ratings yet
- Anatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterDocument75 pagesAnatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterRuth AntolinNo ratings yet
- Great Andamanese Lexicon EnglishDocument65 pagesGreat Andamanese Lexicon EnglishSai VenkateshNo ratings yet
- 12 Cranial Nerves and AssessmentDocument9 pages12 Cranial Nerves and AssessmentRella QuelNo ratings yet
- SONAC-Aqua Feed MarketDocument4 pagesSONAC-Aqua Feed MarketDiel MichNo ratings yet
- Blood DopingDocument16 pagesBlood Dopingpriyanka lalwaniNo ratings yet
- Year 9 Term 2 Science Formative AssessmentDocument2 pagesYear 9 Term 2 Science Formative AssessmentAditya N WardhanaNo ratings yet
- Cholesterol Mortality Chart PDFDocument1 pageCholesterol Mortality Chart PDFTms Arn100% (1)
- Chapter 19 - Lymphatic System and ImmunityDocument68 pagesChapter 19 - Lymphatic System and ImmunityAurea Nazaire100% (2)
- D 5 LRDocument2 pagesD 5 LRDianelie BacenaNo ratings yet
- Ocw Humanos y Otros AnimalesDocument4 pagesOcw Humanos y Otros Animalesmiguel6789No ratings yet
- Arthro 1Document55 pagesArthro 1MenDel Icj IcjiNo ratings yet
- Venomous Snakes of IraqDocument5 pagesVenomous Snakes of IraqLisa3000No ratings yet
- Asphyxia 2Document55 pagesAsphyxia 2api-19916399100% (1)
- Schirmer TestDocument3 pagesSchirmer TestRisa UtamiNo ratings yet
- Pasteurization of Mother's Own Milk Reduces Fat Absorption and Growth in Preterm InfantsDocument5 pagesPasteurization of Mother's Own Milk Reduces Fat Absorption and Growth in Preterm InfantsDianne Faye ManabatNo ratings yet
- Animal Experimentation ViewpointsDocument80 pagesAnimal Experimentation ViewpointschristianbarrigaNo ratings yet
- Dengue Case PresDocument49 pagesDengue Case PresDee SarajanNo ratings yet
- Abnormal Uterine ActionDocument64 pagesAbnormal Uterine ActionKanimozhi Kasinathan100% (1)
- Multiple AlleleDocument19 pagesMultiple AlleleAllen Nanqui DadizonNo ratings yet
- Breast Care in BreastfeedingDocument11 pagesBreast Care in BreastfeedingBella Cy LopezNo ratings yet
- Automated Cell Counts HB Estimation MethodsDocument10 pagesAutomated Cell Counts HB Estimation Methodsjohn mwambuNo ratings yet
- Key Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !Document6 pagesKey Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !June DumdumayaNo ratings yet
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmGabriella AguirreNo ratings yet
- Down SexDocument14 pagesDown SexRuslan ZhuravskyNo ratings yet
- A Case of Subcorneal Pustular Dermatosis Successfully Treated With AcitretinDocument3 pagesA Case of Subcorneal Pustular Dermatosis Successfully Treated With Acitretindr_RMNo ratings yet
- Ilocos Sur Community College: Barangay ChairmanDocument3 pagesIlocos Sur Community College: Barangay ChairmanJorge DanielleNo ratings yet
- Studi Deskriptif Mengenai Resiliensi Pada ODHA Di Komunitas KDS Puzzle Club BandungDocument7 pagesStudi Deskriptif Mengenai Resiliensi Pada ODHA Di Komunitas KDS Puzzle Club BandungArif GustyawanNo ratings yet