You might also like
- 3096 3113985 Flash Mobber Info 2024Document1 page3096 3113985 Flash Mobber Info 2024MelissaNo ratings yet
- CompPlan Certified US-ENDocument1 pageCompPlan Certified US-ENMelissaNo ratings yet
- 1 Patient FloatDocument2 pages1 Patient FloatMelissaNo ratings yet
- Keys To Nursing Success Chapter 1Document42 pagesKeys To Nursing Success Chapter 1Melissa100% (2)
- Benefits SummaryDocument27 pagesBenefits SummaryMelissaNo ratings yet
- Position on assisting with medicationsDocument2 pagesPosition on assisting with medicationsMelissaNo ratings yet
- Nursing Management Concept MapDocument1 pageNursing Management Concept MapXy-Za Roy Marie100% (1)
- 2023 R1 USEN ConsultantGuide 4webDocument28 pages2023 R1 USEN ConsultantGuide 4webMelissaNo ratings yet
- (Regular/Irregular) Location:: Cardiovascular: GenitourinaryDocument1 page(Regular/Irregular) Location:: Cardiovascular: GenitourinaryMelissaNo ratings yet
- 25 Psychiatric Nursing Mnemonics and Tricks - NurseBuffDocument24 pages25 Psychiatric Nursing Mnemonics and Tricks - NurseBuffMelissa100% (3)
- Keys To Nursing Success Chapter 2Document32 pagesKeys To Nursing Success Chapter 2MelissaNo ratings yet
- Keys To Nursing Success Chapter 3Document34 pagesKeys To Nursing Success Chapter 3MelissaNo ratings yet
- Nursing ProcessDocument1 pageNursing ProcessMelissaNo ratings yet
- The Complexities of Care: Nursing Reconsidered: Edited by Sioban Nelson and Suzanne GordonDocument0 pagesThe Complexities of Care: Nursing Reconsidered: Edited by Sioban Nelson and Suzanne GordonMelissaNo ratings yet
- Personality Disorders - PartyDocument3 pagesPersonality Disorders - PartyMelissaNo ratings yet
- hippocrateshipaaII PDFDocument8 pageshippocrateshipaaII PDFMelissaNo ratings yet
- Chart 40-9Document1 pageChart 40-9MelissaNo ratings yet
- PDFDocument6 pagesPDFMelissaNo ratings yet
- Chart 40-8Document1 pageChart 40-8MelissaNo ratings yet
- Differential Diagnosis of Chest Pain ChartDocument1 pageDifferential Diagnosis of Chest Pain ChartMelissaNo ratings yet
- Increased Oxygen Demand and Decreased Supply FactorsDocument1 pageIncreased Oxygen Demand and Decreased Supply FactorsMelissaNo ratings yet
- Chest Pain Causes ChartDocument1 pageChest Pain Causes ChartMelissaNo ratings yet
- Chart 38-8Document1 pageChart 38-8MelissaNo ratings yet
- Genetic Considerations For Hypercholesterolemia: Unit 8Document1 pageGenetic Considerations For Hypercholesterolemia: Unit 8MelissaNo ratings yet
- Laboratory Test Goals to Prevent CADDocument1 pageLaboratory Test Goals to Prevent CADMelissaNo ratings yet
- Nursing ProcessDocument1 pageNursing ProcessMelissaNo ratings yet
- Causes of Intimal Vessel Wall Injury: CHART 40-2Document1 pageCauses of Intimal Vessel Wall Injury: CHART 40-2MelissaNo ratings yet
- AV Block Dysrhythmias GuideDocument2 pagesAV Block Dysrhythmias GuideMelissaNo ratings yet
- Ventricular Dysrhythmias: Etiology, Physical Assessment, and TreatmentDocument2 pagesVentricular Dysrhythmias: Etiology, Physical Assessment, and TreatmentMelissaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Buy Adderall 5 MG OnlineDocument11 pagesBuy Adderall 5 MG OnlineAdderall UsaNo ratings yet
- PH150 Final Exam ReviewDocument14 pagesPH150 Final Exam ReviewNongre ArphonNo ratings yet
- The Importance of Physical FitnessDocument6 pagesThe Importance of Physical FitnessHayate TsukadaNo ratings yet
- KayelarasiDocument109 pagesKayelarasivallabhaneni rajeshNo ratings yet
- CastDocument12 pagesCastJohn AlanoNo ratings yet
- Glossary For Basic Occupational Safety and Health English 17 11 2014Document20 pagesGlossary For Basic Occupational Safety and Health English 17 11 2014FIDO DIDONo ratings yet
- Pediatric Red Ear Syndrome: A Case Report of An Erythromelalgia Type and Review of The LiteratureDocument4 pagesPediatric Red Ear Syndrome: A Case Report of An Erythromelalgia Type and Review of The LiteraturedanniwebbNo ratings yet
- What Is StressDocument9 pagesWhat Is StressUsamaNo ratings yet
- Isk IiDocument70 pagesIsk IikafhcompNo ratings yet
- The Effects of Alcohol On The BrainDocument15 pagesThe Effects of Alcohol On The BrainAndreea PetreaNo ratings yet
- FIRST AID EDUCATION Part 1 and 2-DESKTOP-MTDTU1RDocument14 pagesFIRST AID EDUCATION Part 1 and 2-DESKTOP-MTDTU1RMary Ann VALLECERNo ratings yet
- The Gynaecologist'S and Obstetrician'S Journal Monthly Continuing Medical Training JournalDocument5 pagesThe Gynaecologist'S and Obstetrician'S Journal Monthly Continuing Medical Training JournalSeulean BogdanNo ratings yet
- Visitation Levels: Green Level Red LevelDocument2 pagesVisitation Levels: Green Level Red LevelKelsey DuncanNo ratings yet
- Dr. Vivek Bindra Bada Business Pvt. LTD: Content Contained Within Is The Sole Proprietary ofDocument6 pagesDr. Vivek Bindra Bada Business Pvt. LTD: Content Contained Within Is The Sole Proprietary ofNISHANT395100% (1)
- Genitourinary TuberculosisDocument15 pagesGenitourinary TuberculosisMrunal Dive100% (1)
- KDIGO GD Guideline Key Takeaways For Clinicians Lupus NephritisDocument1 pageKDIGO GD Guideline Key Takeaways For Clinicians Lupus Nephritisadamu mohammadNo ratings yet
- The Vaccine Adverse Event Reporting System (VAERS)Document21 pagesThe Vaccine Adverse Event Reporting System (VAERS)Kraft DinnerNo ratings yet
- Report Project Osha PDFDocument27 pagesReport Project Osha PDFSky FireNo ratings yet
- E000779 FullDocument19 pagesE000779 Fullmartina silalahiNo ratings yet
- Benefits of Dark Chocolate PDFDocument4 pagesBenefits of Dark Chocolate PDFzulaikha fatinNo ratings yet
- Vertebral Canal, DR Adel Bondok 2022Document3 pagesVertebral Canal, DR Adel Bondok 2022Amira Sobh100% (1)
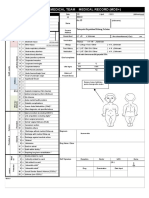
- Emergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplyDocument2 pagesEmergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplySyafiraIdhatunNasyiahNo ratings yet
- Star Health and Allied Insurance Company Limited: Customer Information Sheet - Family Health Optima Insurance PlanDocument12 pagesStar Health and Allied Insurance Company Limited: Customer Information Sheet - Family Health Optima Insurance PlanLokanath ChoudhuryNo ratings yet
- Sillness and Loe Plaque Index 1964Document2 pagesSillness and Loe Plaque Index 1964karthik33% (3)
- Psychiartry NotesDocument38 pagesPsychiartry NotesAlthea Lujille PinazoNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument29 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistslianaidrisNo ratings yet
- Parasitology Material Book (Medical.360°)Document320 pagesParasitology Material Book (Medical.360°)Muhammad Javed Gaba100% (1)
- Raynaud Disease ReportingDocument20 pagesRaynaud Disease ReportingShimri MagsicoNo ratings yet
- Department of Clinical Biochemistry: Creatinine, SerumDocument3 pagesDepartment of Clinical Biochemistry: Creatinine, SerumrishikundanNo ratings yet
- The Lancet NCDI Poverty Commission: Bridging A Gap in Universal Health Coverage For The Poorest BillionDocument54 pagesThe Lancet NCDI Poverty Commission: Bridging A Gap in Universal Health Coverage For The Poorest BillionMario DavilaNo ratings yet