You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Serum Levels of Sex Steroids in Benign and Malignant Disorders of Breast in Libyan Women Full ModelDocument1 pageSerum Levels of Sex Steroids in Benign and Malignant Disorders of Breast in Libyan Women Full ModelJagannadha Rao PeelaNo ratings yet
- Tobacco Exposure and Alcoholic Usage As Risk Factors of Head and Neck CancerDocument6 pagesTobacco Exposure and Alcoholic Usage As Risk Factors of Head and Neck CancerJagannadha Rao PeelaNo ratings yet
- LDH and Gamma GT in Ca Breast in LibyaDocument1 pageLDH and Gamma GT in Ca Breast in LibyaJagannadha Rao PeelaNo ratings yet
- Correlation Between Glycated Hemoglobin and Serum Lipids in Type 2 Diabetics in Eastern LibyaDocument7 pagesCorrelation Between Glycated Hemoglobin and Serum Lipids in Type 2 Diabetics in Eastern LibyaJagannadha Rao PeelaNo ratings yet
- Role of HbA1c and Microalbuminemia in Type2 DMDocument1 pageRole of HbA1c and Microalbuminemia in Type2 DMJagannadha Rao PeelaNo ratings yet
- 'Homocysteine, An Early Predictor of Cardiovascular Risk in Type 2 Diabetes Mellitus "Document4 pages'Homocysteine, An Early Predictor of Cardiovascular Risk in Type 2 Diabetes Mellitus "Jagannadha Rao PeelaNo ratings yet
- Antioxidant Capacity and Lipid PeroxidationDocument1 pageAntioxidant Capacity and Lipid PeroxidationJagannadha Rao PeelaNo ratings yet
- Effect of Piperine On LFT of Non - Transgenic MiceDocument1 pageEffect of Piperine On LFT of Non - Transgenic MiceJagannadha Rao PeelaNo ratings yet
- Serum FSH, LH and Prolactin Levels in Carcinoma Breast of Libyan WomenDocument1 pageSerum FSH, LH and Prolactin Levels in Carcinoma Breast of Libyan WomenJagannadha Rao PeelaNo ratings yet
- Correlation Between Glycated Hemoglobin and Type 2 DiabetisDocument1 pageCorrelation Between Glycated Hemoglobin and Type 2 DiabetisJagannadha Rao PeelaNo ratings yet
- Cystatin For AaccDocument1 pageCystatin For AaccJagannadha Rao PeelaNo ratings yet
- Relationship Between Serum Lipids and Breast Cancer in LibyaDocument1 pageRelationship Between Serum Lipids and Breast Cancer in LibyaJagannadha Rao PeelaNo ratings yet
- Homocysteine As A Risk Factor For Atherosclerosis in Type 2 Diabetes MellitusDocument1 pageHomocysteine As A Risk Factor For Atherosclerosis in Type 2 Diabetes MellitusJagannadha Rao PeelaNo ratings yet
- Circulating Levels of Tumor MarkersDocument1 pageCirculating Levels of Tumor MarkersJagannadha Rao PeelaNo ratings yet
- Ferritin As An Indices of Body Iron Stores and Acute Myocardeal Infarction in DiabeticsDocument58 pagesFerritin As An Indices of Body Iron Stores and Acute Myocardeal Infarction in DiabeticsJagannadha Rao PeelaNo ratings yet
- Epidemiology of Bronchial AshtmaDocument3 pagesEpidemiology of Bronchial AshtmaJagannadha Rao PeelaNo ratings yet
- Role of Serum Uric Acid in Carcinoma of Breast in Libyan PatientsDocument2 pagesRole of Serum Uric Acid in Carcinoma of Breast in Libyan PatientsJagannadha Rao PeelaNo ratings yet
- Announcements 06Document13 pagesAnnouncements 06Jagannadha Rao PeelaNo ratings yet
- Jagannadha Rao PeelaDocument2 pagesJagannadha Rao PeelaJagannadha Rao PeelaNo ratings yet
- Prevalence of Hypertension and Its Risk Factors in An Orang Asli Community in Perak, MalaysiaDocument182 pagesPrevalence of Hypertension and Its Risk Factors in An Orang Asli Community in Perak, MalaysiaJagannadha Rao PeelaNo ratings yet
- Serum Uric Acid Levels As An Adjunct To Asses Certain Psychiatric DisordersDocument1 pageSerum Uric Acid Levels As An Adjunct To Asses Certain Psychiatric DisordersJagannadha Rao PeelaNo ratings yet
- Correlation of Lipid Profile in Coronary Heart Disease Patinets in Libya D-76Document2 pagesCorrelation of Lipid Profile in Coronary Heart Disease Patinets in Libya D-76Jagannadha Rao PeelaNo ratings yet
- Comparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsDocument54 pagesComparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsJagannadha Rao PeelaNo ratings yet
- LDH and Gamma GT in Libyan Breast Cancer Patients.Document3 pagesLDH and Gamma GT in Libyan Breast Cancer Patients.Jagannadha Rao PeelaNo ratings yet
- Euromedlab 2013 Abstracts 211 and 219Document103 pagesEuromedlab 2013 Abstracts 211 and 219Jagannadha Rao PeelaNo ratings yet
- Effect of Piperine On Lipid Profile in Non Transgenic MiceDocument4 pagesEffect of Piperine On Lipid Profile in Non Transgenic MiceJagannadha Rao PeelaNo ratings yet
- Myloperoxidase Is Promising and Predicting Risk Marker For Coronary Heart Disease.Document4 pagesMyloperoxidase Is Promising and Predicting Risk Marker For Coronary Heart Disease.Jagannadha Rao PeelaNo ratings yet
- Quantitative Analysis of Gallstones in Libyan Patients PDFDocument8 pagesQuantitative Analysis of Gallstones in Libyan Patients PDFJagannadha Rao PeelaNo ratings yet
- Prevelence of Dislipedemia Among Middle Aged and Elderly Population in Benghazi.Document11 pagesPrevelence of Dislipedemia Among Middle Aged and Elderly Population in Benghazi.Jagannadha Rao PeelaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pass PACES in Single AttemptDocument101 pagesPass PACES in Single AttemptSOMNATHNo ratings yet
- Electrofisiologia Cardiaca Guia Viasual 2 PDFDocument82 pagesElectrofisiologia Cardiaca Guia Viasual 2 PDFMiguel LizarragaNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- 1.conginital Cardiac DefectsDocument39 pages1.conginital Cardiac DefectsJõsëph Jåy MîthNo ratings yet
- Murmurs Made EasyDocument3 pagesMurmurs Made EasyRoop Singh100% (1)
- CHD ModuleDocument204 pagesCHD ModuleKellie RollinsNo ratings yet
- Cardiac MarkersDocument23 pagesCardiac Markerssulastri triNo ratings yet
- ECG Mastery Improving Your ECG Interpretation SkillsDocument23 pagesECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- Diagnostik Dan Tatalaksana Stable CAD - CCSDocument38 pagesDiagnostik Dan Tatalaksana Stable CAD - CCSIno HajrinNo ratings yet
- ECG For Beginners PDFDocument153 pagesECG For Beginners PDFIonut MoisaNo ratings yet
- (02.12) CM Valvular Heart Diseases (TG20) - Anne Gabrielle LiuDocument18 pages(02.12) CM Valvular Heart Diseases (TG20) - Anne Gabrielle LiuMikmik DGNo ratings yet
- 4 714139450849886574 PDFDocument729 pages4 714139450849886574 PDFSharikha Al Mustashrikha Albeirr100% (1)
- Atrial Fibrillation TDDocument6 pagesAtrial Fibrillation TDapi-594366475No ratings yet
- Pericardial Diseases: Acute PericarditisDocument26 pagesPericardial Diseases: Acute PericarditisamsirakNo ratings yet
- CardiologyDocument4 pagesCardiologyArsany NasserNo ratings yet
- ECGforinternsDocument25 pagesECGforinternsusmleusmle86No ratings yet
- Chapter 12 - The HeartDocument6 pagesChapter 12 - The HeartAgnieszka WisniewskaNo ratings yet
- Types of ArrhythmiaDocument10 pagesTypes of ArrhythmiaRonilyn Mae AlvarezNo ratings yet
- Ecg PDFDocument38 pagesEcg PDFKeerthana BalachandiranNo ratings yet
- Thinking About Ecgs (Garcia)Document9 pagesThinking About Ecgs (Garcia)Filip IonescuNo ratings yet
- CVS in PregnancyDocument47 pagesCVS in PregnancyNATTAPAT SANGKAKULNo ratings yet
- Pulseless Arrest Algorithm For Managing VF and Pulseless VTDocument3 pagesPulseless Arrest Algorithm For Managing VF and Pulseless VTLaili CinthiaNo ratings yet
- Nama: Bilqis Inas Nur Hanifah NIM: 021411131041 Obat - Obat Beta BlockersDocument3 pagesNama: Bilqis Inas Nur Hanifah NIM: 021411131041 Obat - Obat Beta BlockersbilqisinasNo ratings yet
- Valvular Heart DiseaseDocument33 pagesValvular Heart Diseasesimran kaurNo ratings yet
- CVS Examination ProformaDocument4 pagesCVS Examination ProformaAnantha KrishnanNo ratings yet
- Journal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantDocument12 pagesJournal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantSebastian ChandraNo ratings yet
- YFT IM Notes 2Document81 pagesYFT IM Notes 2AHMAD ALROWAILYNo ratings yet
- Cardiac Arrhythmias I: Atrioventricular Conduction Disturbances and BradyarrhythmiasDocument73 pagesCardiac Arrhythmias I: Atrioventricular Conduction Disturbances and BradyarrhythmiasVijay GadagiNo ratings yet
- Teatment Guidelines For Medicine and Primary Care (CCS, 2008)Document241 pagesTeatment Guidelines For Medicine and Primary Care (CCS, 2008)Mirza SmajlovićNo ratings yet
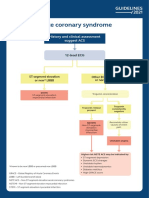
- Acute Coronary Syndrome: History and Clinical Assessment Suggest ACSDocument12 pagesAcute Coronary Syndrome: History and Clinical Assessment Suggest ACSginongNo ratings yet