You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Case Report CHF PedsDocument36 pagesCase Report CHF PedsKanagavalli VijayakumarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Effect of Periodontal Therapy On C-Reactive Protein Levels in Gingival Crevicular Fluid of Patients With Gingivitis and Chronic PeriodontitisDocument5 pagesEffect of Periodontal Therapy On C-Reactive Protein Levels in Gingival Crevicular Fluid of Patients With Gingivitis and Chronic PeriodontitisKanagavalli VijayakumarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Klasifikasi NystagmusDocument5 pagesKlasifikasi NystagmusKanagavalli VijayakumarNo ratings yet
- Toast CriteriaDocument4 pagesToast CriteriaKanagavalli VijayakumarNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- What Is Mindfulness?: Christopher Germer, PH.DDocument6 pagesWhat Is Mindfulness?: Christopher Germer, PH.DolgaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Duros ImplantDocument7 pagesDuros ImplantAri DewiyantiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Understanding POTS - The Invisible IllnessDocument10 pagesUnderstanding POTS - The Invisible IllnessSpencer100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Humanistic PsychologyDocument2 pagesHumanistic PsychologyDillon BrowneNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Effectiveness of Physiotherapy After OperativeDocument3 pagesThe Effectiveness of Physiotherapy After OperativeDanny QuezadaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Comparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFDocument5 pagesComparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFCharina Geofhany DeboraNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Physical Therapy Modalities PDFDocument31 pagesPhysical Therapy Modalities PDFArjun S RajNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Bimasena Menu-And-Price-ListDocument7 pagesBimasena Menu-And-Price-Listbon1ngNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Matary MCQ - 2011 (WWW - Afriqa Sat - Com)Document198 pagesMatary MCQ - 2011 (WWW - Afriqa Sat - Com)Ahmed Attia100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Picmonic NCLEX Study PlanDocument38 pagesPicmonic NCLEX Study PlanHannah Adams73% (33)
- Chapter Outline Overview of Adler's Individual PsychologyDocument2 pagesChapter Outline Overview of Adler's Individual PsychologyNur MNNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Top Communicable Diseases in The Philippines 2019Document4 pagesTop Communicable Diseases in The Philippines 2019Nicole cuencosNo ratings yet
- Obstetric Safety ProtocolsDocument10 pagesObstetric Safety ProtocolsApril LilianNo ratings yet
- 21st Century Cures ActDocument312 pages21st Century Cures ActStephen LoiaconiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- IELTS Reading Choose The HeadingDocument16 pagesIELTS Reading Choose The HeadingPhạm Quốc BảoNo ratings yet
- Case Report VertigoDocument32 pagesCase Report VertigoSuci WulandariNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Israa Hadi ResumeDocument1 pageIsraa Hadi Resumeapi-301344062No ratings yet
- Drug Management of Thyroid DiseaseDocument22 pagesDrug Management of Thyroid DiseaseHassan.shehri100% (6)
- Acute Renal Failure and TreatmentDocument103 pagesAcute Renal Failure and TreatmentNathan AsinasNo ratings yet
- Approach To HeadacheDocument49 pagesApproach To Headachegea pandhita sNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Lidcombe ProgramDocument12 pagesThe Lidcombe ProgramDemosten100% (1)
- Clientele and Audiences in CounselingDocument16 pagesClientele and Audiences in CounselingAzalea Navarra100% (1)
- Torture Treatment Centers - Global Directory 2008Document152 pagesTorture Treatment Centers - Global Directory 2008Coalition for Democracy in IranNo ratings yet
- Pressure Habits, Etiological Factors in MalocclusionDocument1 pagePressure Habits, Etiological Factors in MalocclusionGerardo VacaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
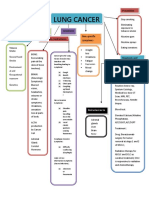
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- Problem With The PowersDocument9 pagesProblem With The PowersNicole Claire LegaspiNo ratings yet
- Amelogenesis Imperfecta Treatment Case ReviewDocument7 pagesAmelogenesis Imperfecta Treatment Case ReviewGeraldo LaurusNo ratings yet
- Hepatic Failure and EncephalopathyDocument4 pagesHepatic Failure and EncephalopathyAnusha VergheseNo ratings yet
- Intracranial Berry Aneurysm - Wikipedia, The Free EncyclopediaDocument3 pagesIntracranial Berry Aneurysm - Wikipedia, The Free EncyclopediaAniket MittalNo ratings yet
- The Effectiveness of Sensory Integration Therapy For Children With AutismDocument16 pagesThe Effectiveness of Sensory Integration Therapy For Children With Autismapi-382628487No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)