You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- PLR CourseDocument43 pagesPLR CourseTaniya ChatterjeeNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
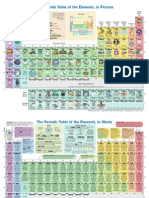
- The Periodic Table of Elements, in PicturesDocument2 pagesThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Observational Studies: Usmle Endpoint StatisticsDocument32 pagesObservational Studies: Usmle Endpoint Statisticskarim khalil100% (1)
- Case Study Myocardial InfarctionDocument23 pagesCase Study Myocardial InfarctionJester GalayNo ratings yet
- How to Relax Effectively with CBT SkillsDocument15 pagesHow to Relax Effectively with CBT SkillsDomingo de LeonNo ratings yet
- PSMDocument62 pagesPSMzamijakaNo ratings yet
- 6 - ADKAR Reinforcement Ebook PDFDocument14 pages6 - ADKAR Reinforcement Ebook PDFHenrique NarcisoNo ratings yet
- RMT TrainningDocument2 pagesRMT TrainningDita Nadya RizkitaNo ratings yet
- OCI Inventario Obsesivo Compulsivo (Foa, 2002)Document11 pagesOCI Inventario Obsesivo Compulsivo (Foa, 2002)Margarita100% (1)
- Masonry QuizDocument12 pagesMasonry QuizJoanne Jose Castro0% (1)
- Hospital Management SystemDocument46 pagesHospital Management SystemDushyant Singh93% (15)
- 3interim Advice For Public Health Authorities On Summer Events MPXDocument6 pages3interim Advice For Public Health Authorities On Summer Events MPXFrancisca BallesterosNo ratings yet
- Joint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Document7 pagesJoint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Francisca BallesterosNo ratings yet
- 2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeDocument11 pages2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeFrancisca BallesterosNo ratings yet
- 5communicable Disease Threats Report 30 Jul 2022 PublicDocument28 pages5communicable Disease Threats Report 30 Jul 2022 PublicFrancisca BallesterosNo ratings yet
- ROA Salmonella-Enteritidis-ST11 2022 FinalDocument19 pagesROA Salmonella-Enteritidis-ST11 2022 FinalFrancisca BallesterosNo ratings yet
- COVID 19 in Children and The Role of School Settings in Transmission Second UpdateDocument37 pagesCOVID 19 in Children and The Role of School Settings in Transmission Second UpdateFrancisca BallesterosNo ratings yet
- Use of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesDocument5 pagesUse of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesFrancisca BallesterosNo ratings yet
- Variable Dictionary VaccineTracker-04!11!2021Document3 pagesVariable Dictionary VaccineTracker-04!11!2021Francisca BallesterosNo ratings yet
- COVID 19 Considerations For Booster Doses in Adolescents Feb 2022Document14 pagesCOVID 19 Considerations For Booster Doses in Adolescents Feb 2022Francisca BallesterosNo ratings yet
- 1considerations For Contact Tracing MPX June 2022Document13 pages1considerations For Contact Tracing MPX June 2022Francisca BallesterosNo ratings yet
- Description and Disclaimer Daily ReportingDocument1 pageDescription and Disclaimer Daily ReportingFrancisca BallesterosNo ratings yet
- Interim Public Health Considerations For COVID 19 Vaccination of AdolescentsDocument19 pagesInterim Public Health Considerations For COVID 19 Vaccination of AdolescentsFrancisca BallesterosNo ratings yet
- 2021-01-13 Variable Dictionary and Disclaimer National Weekly DataDocument1 page2021-01-13 Variable Dictionary and Disclaimer National Weekly DataFrancisca BallesterosNo ratings yet
- Agenda EAAD - European-Level Launch EventDocument1 pageAgenda EAAD - European-Level Launch EventFrancisca BallesterosNo ratings yet
- Hiv and Aids: Surveillance ReportDocument7 pagesHiv and Aids: Surveillance ReportFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 16 Jun 2018Document11 pagesCommunicable Disease Threats Report 16 Jun 2018Francisca BallesterosNo ratings yet
- ECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyDocument1 pageECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyFrancisca BallesterosNo ratings yet
- Variable Dictionary VaccineTracker-20-08-2021Document3 pagesVariable Dictionary VaccineTracker-20-08-2021Francisca BallesterosNo ratings yet
- Zika Virus Safety of Substances of Human Origin Update 2017 WebDocument35 pagesZika Virus Safety of Substances of Human Origin Update 2017 WebFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 26 Aug 2017Document9 pagesCommunicable Disease Threats Report 26 Aug 2017Francisca BallesterosNo ratings yet
- Antimicrobial Resistance Europe 2015Document120 pagesAntimicrobial Resistance Europe 2015Francisca BallesterosNo ratings yet
- ECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEADocument1 pageECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEAFrancisca BallesterosNo ratings yet
- ECDC - ECDC Policy Briefing - Preparing For Zika in The EUDocument1 pageECDC - ECDC Policy Briefing - Preparing For Zika in The EUFrancisca BallesterosNo ratings yet
- Ecdc Infographics2015 Measles Is SeriousDocument1 pageEcdc Infographics2015 Measles Is SeriousFrancisca BallesterosNo ratings yet
- Who Ccsivd Meetingreport SangreDocument31 pagesWho Ccsivd Meetingreport SangreFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 29 Jul 2017Document13 pagesCommunicable Disease Threats Report 29 Jul 2017Francisca BallesterosNo ratings yet
- ECDC Policy BriefingsDocument1 pageECDC Policy BriefingsFrancisca BallesterosNo ratings yet
- ECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsDocument2 pagesECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsFrancisca BallesterosNo ratings yet
- ECDC Epidemiological SituationDocument1 pageECDC Epidemiological SituationFrancisca BallesterosNo ratings yet
- Digestive System Parts PacketDocument2 pagesDigestive System Parts PacketRusherNo ratings yet
- HezekiahWalters Plans 3Document34 pagesHezekiahWalters Plans 3Chris VaughnNo ratings yet
- Name: Jaanvi Mahajan Course: 2ballb Hons. REGISTRATION NO.: 22212033 Subject: Law and Medicine Submitted To: Mrs. Vijaishree Dubey PandeyDocument9 pagesName: Jaanvi Mahajan Course: 2ballb Hons. REGISTRATION NO.: 22212033 Subject: Law and Medicine Submitted To: Mrs. Vijaishree Dubey Pandeyjaanvi mahajanNo ratings yet
- Rhetorical Analysis Revision Final ProjectDocument13 pagesRhetorical Analysis Revision Final Projectapi-371084574100% (1)
- Truvivity by NutriliteDocument10 pagesTruvivity by Nutriliteโยอันนา ยุนอา แคทเธอรีน เอี่ยมสุวรรณNo ratings yet
- Full Download Test Bank For Pharmacology 9th Edition by Mccuistion PDF Full ChapterDocument36 pagesFull Download Test Bank For Pharmacology 9th Edition by Mccuistion PDF Full Chapterpotshardmonied5cuc100% (19)
- Bakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TDocument46 pagesBakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TAlif NakyukoNo ratings yet
- Malmstrom Et Al - 1999 - Oral Montelukast, Inhaled Beclomethasone, and Placebo For Chronic AsthmaDocument10 pagesMalmstrom Et Al - 1999 - Oral Montelukast, Inhaled Beclomethasone, and Placebo For Chronic AsthmaRutvik ShahNo ratings yet
- Antibiotics For Research Applications - BioFiles Issue 4.3Document24 pagesAntibiotics For Research Applications - BioFiles Issue 4.3Sigma-AldrichNo ratings yet
- Material Safety Data Sheet: Section 1 - Product InformationDocument2 pagesMaterial Safety Data Sheet: Section 1 - Product Informationmohamed AdelNo ratings yet
- Mynvax PDF File Contained StandardsDocument1 pageMynvax PDF File Contained StandardsSelvabala904260No ratings yet
- TB Radiology Basic Presentation SlidesDocument72 pagesTB Radiology Basic Presentation SlidesSherwin ManuekeNo ratings yet
- History + Mission +SWOTDocument2 pagesHistory + Mission +SWOThangchan_superchibiNo ratings yet
- NEWCROSS Site Survey - Rev1Document37 pagesNEWCROSS Site Survey - Rev1eke23No ratings yet
- ACADEMIC CALENDAR MEDICAL PROGRAMME 2019/2020Document1 pageACADEMIC CALENDAR MEDICAL PROGRAMME 2019/2020AnNourNo ratings yet
- Pediatrics ArimgsasDocument403 pagesPediatrics ArimgsasGabriela ChristianNo ratings yet
- Planning Design and Analysis of G+1 Hospital Building For Iiit Srikakulam CampusDocument1 pagePlanning Design and Analysis of G+1 Hospital Building For Iiit Srikakulam CampusSaritha TejavathNo ratings yet
- Nursing responsibilities for tramadol administrationDocument2 pagesNursing responsibilities for tramadol administrationThrinNo ratings yet
- DSMDocument2 pagesDSMOtilia EmaNo ratings yet
- The Ethical Dilemma of a Patient's Suicide AttemptDocument2 pagesThe Ethical Dilemma of a Patient's Suicide AttemptgabiiNo ratings yet