You might also like
- Eyfs Planning Examples PackDocument34 pagesEyfs Planning Examples Pack*_niomi_*100% (5)
- The Very Hungry Caterpillar Lesson PlanDocument3 pagesThe Very Hungry Caterpillar Lesson Planapi-291353197No ratings yet
- National Clinical Guideline No. 5 Clinical Handover Nov2014Document306 pagesNational Clinical Guideline No. 5 Clinical Handover Nov2014Ahmad JuliadiNo ratings yet
- CHOP Nursing Shared Governance Structure Ensures Quality Patient CareDocument18 pagesCHOP Nursing Shared Governance Structure Ensures Quality Patient CareHendra HefaNo ratings yet
- TransitionDocument13 pagesTransitionDonna NituraNo ratings yet
- Nurse Residency Program 1Document5 pagesNurse Residency Program 1api-315956703No ratings yet
- Journal of Medical Ethics and History of Medicine: Original ArticleDocument11 pagesJournal of Medical Ethics and History of Medicine: Original Articleali sarjunipadangNo ratings yet
- Hand Off CommunicationDocument6 pagesHand Off CommunicationALELAW100% (1)
- Presentor-: Ruma Sen: MN (Previous) RakconDocument40 pagesPresentor-: Ruma Sen: MN (Previous) Rakconcy100% (1)
- PROJECT CHARTER Pressure UlcerDocument2 pagesPROJECT CHARTER Pressure UlcerQuality PmnhNo ratings yet
- CQE 7 Nursing Quality Indicators 1Document24 pagesCQE 7 Nursing Quality Indicators 1Inder Singh YadavNo ratings yet
- Mod2 - Ch3 - Health IndicatorsDocument13 pagesMod2 - Ch3 - Health IndicatorsSara Sunabara100% (1)
- IHI Patient Family Experience of Hospital Care White Paper 2011Document34 pagesIHI Patient Family Experience of Hospital Care White Paper 2011Sorina VoicuNo ratings yet
- National Medication Safety Guidelines Manual FinalDocument29 pagesNational Medication Safety Guidelines Manual FinalNur HidayatiNo ratings yet
- Medical Records: Standard MOI.9Document5 pagesMedical Records: Standard MOI.9Azza FaroukNo ratings yet
- Patient Safety Indicator PDFDocument149 pagesPatient Safety Indicator PDFDang RajoNo ratings yet
- Clinical Area Objective Headnursing Activities Students Activities EvaluationDocument2 pagesClinical Area Objective Headnursing Activities Students Activities EvaluationTrixie Anne GamotinNo ratings yet
- Interdisciplinary Nursing DocumentationDocument6 pagesInterdisciplinary Nursing Documentationgrace_nakateNo ratings yet
- Brochure NursingDocument10 pagesBrochure Nursingsiska dwiNo ratings yet
- ENA Leadership Conference 2013 ProgramDocument17 pagesENA Leadership Conference 2013 ProgramEmergency Nurses AssociationNo ratings yet
- Understanding Holistic NursingDocument46 pagesUnderstanding Holistic NursingadeNo ratings yet
- What Is Administration in Nursing Service?Document4 pagesWhat Is Administration in Nursing Service?Princess Melanie MelendezNo ratings yet
- CPL Self-Assessment ToolDocument7 pagesCPL Self-Assessment Toolapi-533585410No ratings yet
- Clinical Establishment Act Standards For Hospital (LEVEL 3)Document36 pagesClinical Establishment Act Standards For Hospital (LEVEL 3)bksubrat100% (3)
- SN JDDocument2 pagesSN JDChoi ToNo ratings yet
- QI in Nursing 2012Document10 pagesQI in Nursing 2012rnrmmanphdNo ratings yet
- Advanced Nursing Process Quality Comparing The International Classi Cation For Nursing Practice (ICNP) With The NANDAInternational (NANDA-I) and Nursing Interventions Classi Cation (NIC)Document9 pagesAdvanced Nursing Process Quality Comparing The International Classi Cation For Nursing Practice (ICNP) With The NANDAInternational (NANDA-I) and Nursing Interventions Classi Cation (NIC)Fitra PringgayudaNo ratings yet
- Ways To Improve The Health SystemDocument18 pagesWays To Improve The Health SystemB I N SNo ratings yet
- Capstone Clinical Nursing JudgementDocument7 pagesCapstone Clinical Nursing Judgementapi-544889322No ratings yet
- Qi Nursing Communication Final - Nurs 484Document12 pagesQi Nursing Communication Final - Nurs 484api-558100249No ratings yet
- Letter of RecommendationDocument1 pageLetter of RecommendationShàhríàrõ Dã Ràkínskì100% (1)
- DLL For Catch Up Friday Homeroom Guidance January 19Document2 pagesDLL For Catch Up Friday Homeroom Guidance January 19marinella.boridasNo ratings yet
- A Learning Model For NursingDocument7 pagesA Learning Model For NursingLina Mahayaty SembiringNo ratings yet
- Emergency Nurses Association (ENA)Document5 pagesEmergency Nurses Association (ENA)Ngu W PhooNo ratings yet
- Nursing InformaticsDocument1 pageNursing InformaticsStacey GarciaNo ratings yet
- Standard of Nursing ServicesDocument30 pagesStandard of Nursing Servicesardian_primaNo ratings yet
- Nursing Competencies. The Artristy of NursingDocument6 pagesNursing Competencies. The Artristy of NursingneoclintNo ratings yet
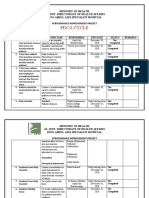
- Pdca CycleDocument4 pagesPdca CycleHamid BouleghabNo ratings yet
- Critical ThinkingDocument7 pagesCritical ThinkingAru VermaNo ratings yet
- Formulation: Vision and Mission: Session 2 Ratna Roostika, PHDDocument25 pagesFormulation: Vision and Mission: Session 2 Ratna Roostika, PHDAnonymous iiWoac8kNo ratings yet
- Pre Test Acept 2014Document5 pagesPre Test Acept 2014Hani TuasikalNo ratings yet
- Situational Leadership ModelDocument5 pagesSituational Leadership ModelHani TuasikalNo ratings yet
- File Test 1 B Answer Key: Grammar, Vocabulary, and PronunciationDocument3 pagesFile Test 1 B Answer Key: Grammar, Vocabulary, and PronunciationB McNo ratings yet
- Evidencebased Healthcare and Quality ImprovementDocument8 pagesEvidencebased Healthcare and Quality ImprovementJemimah BureresNo ratings yet
- Data CollectionDocument30 pagesData CollectionHarihara PuthiranNo ratings yet
- L & M in Nursing - ConflictDocument26 pagesL & M in Nursing - ConflictMichael SamaniegoNo ratings yet
- Conflict Management: Literature ReviewDocument6 pagesConflict Management: Literature ReviewNivedkrishna ThavarayilNo ratings yet
- Seminar PresentationDocument31 pagesSeminar Presentationapi-520940649No ratings yet
- Nursing Sensitive Indicators Their RoleDocument3 pagesNursing Sensitive Indicators Their RolePuspita Eka Kurnia SariNo ratings yet
- Enhancing Nurses Pain Assessment To Improve.11Document2 pagesEnhancing Nurses Pain Assessment To Improve.11Na d'Nazaie CodeNo ratings yet
- Falls Screeening in ChildrenDocument13 pagesFalls Screeening in ChildrenLovi Krissadi100% (1)
- Joint Commission Tracers 2011: What Hospitals Need to KnowDocument38 pagesJoint Commission Tracers 2011: What Hospitals Need to Knowpathoslmc globalNo ratings yet
- Hospital Registration and Billing System Layout GuideDocument4 pagesHospital Registration and Billing System Layout GuideSthitapragyan senapatiNo ratings yet
- Quality and Patient SafetyDocument19 pagesQuality and Patient SafetyRekhaNo ratings yet
- Patient Safety: What Should We Be Trying To Communicate?Document32 pagesPatient Safety: What Should We Be Trying To Communicate?cicaklomenNo ratings yet
- Quality Improvement Manager in Northwest Indiana Resume Nancy WulffDocument2 pagesQuality Improvement Manager in Northwest Indiana Resume Nancy WulffNancy WulffNo ratings yet
- Nur 490w BcaDocument9 pagesNur 490w Bcaapi-369824515100% (1)
- Marketing Mix - The 4 P's of Marketing ExplainedDocument6 pagesMarketing Mix - The 4 P's of Marketing ExplainedDeepak Kalonia JangraNo ratings yet
- Identifying Patient Safety PrioritiesDocument10 pagesIdentifying Patient Safety PrioritiesReybs -isabella CalubNo ratings yet
- Nurse Turnover A Literature ReviewDocument27 pagesNurse Turnover A Literature ReviewRima FutihasariNo ratings yet
- Monograph of Qi ProjectDocument29 pagesMonograph of Qi ProjectmerahiNo ratings yet
- The Dangers of ComplacencyDocument3 pagesThe Dangers of Complacencyegahmulia100% (2)
- 2007 International Patient Safety GoalsDocument1 page2007 International Patient Safety GoalsElias Baraket FreijyNo ratings yet
- Assingnment 3 775Document17 pagesAssingnment 3 775madhwa79No ratings yet
- ISOBAR Clinical HandoverDocument3 pagesISOBAR Clinical HandoverSamer FarhanNo ratings yet
- Final Quality Improvement PaperDocument8 pagesFinal Quality Improvement Paperapi-251822043No ratings yet
- Inpatient Patient ExperienceDocument12 pagesInpatient Patient ExperienceRodrigoSachiFreitasNo ratings yet
- TLXScaleDocument1 pageTLXScalespidey2000No ratings yet
- Quality, safety and EBP glossary 2012Document6 pagesQuality, safety and EBP glossary 2012Hani TuasikalNo ratings yet
- Malaysia Scholarship 201Document184 pagesMalaysia Scholarship 201Hani TuasikalNo ratings yet
- Scholarships UKDocument412 pagesScholarships UKHani TuasikalNo ratings yet
- Scholarships UKDocument412 pagesScholarships UKHani TuasikalNo ratings yet
- Absens IDocument2 pagesAbsens IHani TuasikalNo ratings yet
- Quality, safety and EBP glossary 2012Document6 pagesQuality, safety and EBP glossary 2012Hani TuasikalNo ratings yet
- Referensi Jurnal Rotavirus BMCDocument7 pagesReferensi Jurnal Rotavirus BMCFerry GhifariNo ratings yet
- Gambaran Pelaksanaan Unversal LimbahDocument6 pagesGambaran Pelaksanaan Unversal LimbahHani TuasikalNo ratings yet
- Machine Methode: Diagram FishboneDocument1 pageMachine Methode: Diagram FishboneHani TuasikalNo ratings yet
- Gambaran Pelaksanaan Unversal LimbahDocument6 pagesGambaran Pelaksanaan Unversal LimbahHani TuasikalNo ratings yet
- 2793 2783 1 PBDocument9 pages2793 2783 1 PBHani TuasikalNo ratings yet
- Massage Therapy For Osteoarthritis of The KneeDocument6 pagesMassage Therapy For Osteoarthritis of The KneeDrAbhay ShankargoudaNo ratings yet
- Elderly Knee Pain StudyDocument6 pagesElderly Knee Pain StudyHani TuasikalNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Hani TuasikalNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Hani TuasikalNo ratings yet
- Jadwal Test TOEFL PDFDocument13 pagesJadwal Test TOEFL PDFHani TuasikalNo ratings yet
- OSU Equity & Diversity in EducationDocument18 pagesOSU Equity & Diversity in EducationCampus ReformNo ratings yet
- Aboriginal Unit of WorkDocument30 pagesAboriginal Unit of Workapi-321113223No ratings yet
- My StoryDocument11 pagesMy Storyvithai zaraunkarNo ratings yet
- Personal Value and Job Satisfaction of Private B.Ed. College TeachersDocument8 pagesPersonal Value and Job Satisfaction of Private B.Ed. College TeachersEditor IJTSRDNo ratings yet
- 1 Online MBA, Financial Times 2017Document36 pages1 Online MBA, Financial Times 2017veda20No ratings yet
- Critical Literacy Lesson PlanDocument9 pagesCritical Literacy Lesson PlanJuanCa MonteneGroNo ratings yet
- Research MethodologyDocument2 pagesResearch MethodologyGuruPrasad MNo ratings yet
- ATC Strategic Plan 2020-2025Document24 pagesATC Strategic Plan 2020-2025Brandon LuciusNo ratings yet
- Aiou 8601 A1Document18 pagesAiou 8601 A1Khan BachaNo ratings yet
- Brooklyn Nine Lesson TwoDocument2 pagesBrooklyn Nine Lesson Twoapi-218334420100% (1)
- To All Tle Teacher LetterDocument7 pagesTo All Tle Teacher Letteralvin n. vedarozagaNo ratings yet
- Registration Form For AMO Contest: RegisrtationDocument2 pagesRegistration Form For AMO Contest: RegisrtationWu XinNo ratings yet
- Promoting ICT Education in Developing Countries CaDocument8 pagesPromoting ICT Education in Developing Countries CaELLEN CERNANo ratings yet
- Christie Resume 2014Document2 pagesChristie Resume 2014api-259523809No ratings yet
- Grade 7 Sample Lesson Plan: Unit 2 - Physical Activity and Stress ManagementDocument2 pagesGrade 7 Sample Lesson Plan: Unit 2 - Physical Activity and Stress ManagementJun Dl CrzNo ratings yet
- Understanding Juvenile DelinquencyDocument10 pagesUnderstanding Juvenile DelinquencyMustain RahmanNo ratings yet
- 5E Lesson PlanDocument1 page5E Lesson PlanNieva Mae MartinezNo ratings yet
- OutcomesDocument52 pagesOutcomesapi-316034054No ratings yet
- FS 2 - Episode 2 Intended Learning Outcomes Lesson Objectives As My Guiding StarDocument12 pagesFS 2 - Episode 2 Intended Learning Outcomes Lesson Objectives As My Guiding StarHenry Kahal Orio Jr.No ratings yet
- Deconstruct What Speakers Great DoDocument2 pagesDeconstruct What Speakers Great DoAiman OthmanNo ratings yet
- Unit 3 (WPH03) June 2014Document21 pagesUnit 3 (WPH03) June 2014Web BooksNo ratings yet
- Learning Plans in The Context of The 21 CenturyDocument62 pagesLearning Plans in The Context of The 21 CenturyAnna Rica SicangNo ratings yet
- State Examples The Importance of Plants To Humans and AnimalsDocument3 pagesState Examples The Importance of Plants To Humans and Animalsnorma annuarNo ratings yet
- Request Letter For The School HeadDocument1 pageRequest Letter For The School HeadMart NulazNo ratings yet