You might also like
- Principles and Applications of Clinical Mass Spectrometry: Small Molecules, Peptides, and PathogensFrom EverandPrinciples and Applications of Clinical Mass Spectrometry: Small Molecules, Peptides, and PathogensNader RifaiNo ratings yet
- Microbiology and Molecular Diagnosis in Pathology: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeFrom EverandMicrobiology and Molecular Diagnosis in Pathology: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeNo ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- Safe Blood: Purifying the Nations Blood Supply in the Age of AFrom EverandSafe Blood: Purifying the Nations Blood Supply in the Age of ANo ratings yet
- Agglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4From EverandAgglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4No ratings yet
- Tietz's Applied Laboratory MedicineFrom EverandTietz's Applied Laboratory MedicineMitchell G. ScottRating: 3 out of 5 stars3/5 (1)
- IMMUNOHEMATOLOGY AND BLOOD BANKING: Passbooks Study GuideFrom EverandIMMUNOHEMATOLOGY AND BLOOD BANKING: Passbooks Study GuideRating: 1 out of 5 stars1/5 (1)
- Senior Medical Laboratory Technician: Passbooks Study GuideFrom EverandSenior Medical Laboratory Technician: Passbooks Study GuideNo ratings yet
- Clinical Chemistry, Immunology and Laboratory Quality Control: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeFrom EverandClinical Chemistry, Immunology and Laboratory Quality Control: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeRating: 5 out of 5 stars5/5 (1)
- Urinalysis and Body Fluids for Cls & MltFrom EverandUrinalysis and Body Fluids for Cls & MltNo ratings yet
- Transfusion Medicine for Pathologists: A Comprehensive Review for Board Preparation, Certification, and Clinical PracticeFrom EverandTransfusion Medicine for Pathologists: A Comprehensive Review for Board Preparation, Certification, and Clinical PracticeRating: 3 out of 5 stars3/5 (1)
- Handbook of Transfusion MedicineFrom EverandHandbook of Transfusion MedicineChristopher HillyerRating: 4 out of 5 stars4/5 (4)
- Medical Laboratory Technician Career JournalDocument2 pagesMedical Laboratory Technician Career Journalapi-406104878100% (1)
- Introduction to Medical Laboratory TechnologyFrom EverandIntroduction to Medical Laboratory TechnologyRating: 2.5 out of 5 stars2.5/5 (7)
- Code of Ethics Guidance DocumentDocument30 pagesCode of Ethics Guidance DocumentASHVINBHAI VACHHANI100% (1)
- Transfusion Medicine and Hemostasis: Clinical and Laboratory AspectsFrom EverandTransfusion Medicine and Hemostasis: Clinical and Laboratory AspectsRating: 4 out of 5 stars4/5 (9)
- Mls Imls Reading ListDocument3 pagesMls Imls Reading ListPeng KwanNo ratings yet
- Introduction of Clinical BiochemistryDocument32 pagesIntroduction of Clinical BiochemistryKaren LowNo ratings yet
- Quality Control2Document32 pagesQuality Control2Mustafa KhandgawiNo ratings yet
- Transfusion Medicine, Apheresis, and Hemostasis: Review Questions and Case StudiesFrom EverandTransfusion Medicine, Apheresis, and Hemostasis: Review Questions and Case StudiesRating: 5 out of 5 stars5/5 (2)
- TextbookReferenceList MLA 2017Document3 pagesTextbookReferenceList MLA 2017APNo ratings yet
- Board of Directors: Ascp-Ascp Certification & Qualification Comparison ChartDocument1 pageBoard of Directors: Ascp-Ascp Certification & Qualification Comparison ChartMustaffah KabelyyonNo ratings yet
- Clinical Chemistry - Theory, Analysis, CorrelationDocument344 pagesClinical Chemistry - Theory, Analysis, Correlationaristides.quinteroNo ratings yet
- FlaggingDocument65 pagesFlaggingTony KurniawanNo ratings yet
- Accurate Results in the Clinical Laboratory: A Guide to Error Detection and CorrectionFrom EverandAccurate Results in the Clinical Laboratory: A Guide to Error Detection and CorrectionRating: 5 out of 5 stars5/5 (1)
- ML7111 MCQs Answers Sep 2019Document10 pagesML7111 MCQs Answers Sep 2019Cleo Salvador100% (2)
- Ascp International Procedures BookDocument25 pagesAscp International Procedures BookDegee O. Gonzales100% (1)
- ABO DiscrepanicesDocument12 pagesABO DiscrepanicesGlenn PerezNo ratings yet
- Essentials of ABO -Rh Grouping and Compatibility Testing: Theoretical Aspects and Practical ApplicationFrom EverandEssentials of ABO -Rh Grouping and Compatibility Testing: Theoretical Aspects and Practical ApplicationRating: 5 out of 5 stars5/5 (1)
- Self-assessment Q&A in Clinical Laboratory Science, IIIFrom EverandSelf-assessment Q&A in Clinical Laboratory Science, IIIRating: 3 out of 5 stars3/5 (1)
- Lab Policies Complete Blood Count of Whole Blood On The Sysmex KX 21N - RB Lab 1535Document20 pagesLab Policies Complete Blood Count of Whole Blood On The Sysmex KX 21N - RB Lab 1535tomNo ratings yet
- CSMLS C2 QuestionsDocument49 pagesCSMLS C2 QuestionsApollo Ochieng100% (1)
- Pathogenesis, Treatment and Prevention of LeishmaniasisFrom EverandPathogenesis, Treatment and Prevention of LeishmaniasisMukesh SamantNo ratings yet
- Hematology and Coagulation: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeFrom EverandHematology and Coagulation: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeNo ratings yet
- Laboratory Quality ControlDocument63 pagesLaboratory Quality Control"DocAxi" Maximo B Axibal Jr MD FPSPNo ratings yet
- Techniques in Clinical Chemistry: A Handbook for Medical Laboratory TechniciansFrom EverandTechniques in Clinical Chemistry: A Handbook for Medical Laboratory TechniciansNo ratings yet
- I JomedDocument23 pagesI JomedSafiqulatif AbdillahNo ratings yet
- I JomedDocument23 pagesI JomedSafiqulatif AbdillahNo ratings yet
- Guide To Surgical Site MarkingDocument24 pagesGuide To Surgical Site MarkingSafiqulatif AbdillahNo ratings yet
- 4612 Early Warning Score (June 2013)Document8 pages4612 Early Warning Score (June 2013)Safiqulatif AbdillahNo ratings yet
- VentilationDocument7 pagesVentilationDodowi CspogNo ratings yet
- 10 Facts On Patient SafetyDocument3 pages10 Facts On Patient SafetySafiqulatif AbdillahNo ratings yet
- QPS Sample GuidelinesDocument23 pagesQPS Sample GuidelinesSafiqulatif AbdillahNo ratings yet
- SkriningDocument6 pagesSkriningSafiqulatif AbdillahNo ratings yet
- Preventing Patient ReboundsDocument11 pagesPreventing Patient ReboundsSafiqulatif AbdillahNo ratings yet
- Reducing Hospital ReadmissionDocument6 pagesReducing Hospital ReadmissionSafiqulatif AbdillahNo ratings yet
- Policy Critical ResultDocument6 pagesPolicy Critical ResultSafiqulatif AbdillahNo ratings yet
- Preventing Patient ReboundsDocument11 pagesPreventing Patient ReboundsSafiqulatif AbdillahNo ratings yet
- Cdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008Document158 pagesCdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008fuentenatura100% (1)
- PPI Di HD Versi CDCDocument63 pagesPPI Di HD Versi CDCSafiqulatif AbdillahNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Governance Board Manual QualityDocument22 pagesGovernance Board Manual QualitySafiqulatif AbdillahNo ratings yet
- Board Committees and TOR QPS CommitteeDocument44 pagesBoard Committees and TOR QPS CommitteeSafiqulatif AbdillahNo ratings yet
- TOI Breaking Bad NewsDocument15 pagesTOI Breaking Bad NewsSafiqulatif AbdillahNo ratings yet
- 2013-2014 Clinical Pathway ApplicationDocument7 pages2013-2014 Clinical Pathway ApplicationSafiqulatif AbdillahNo ratings yet
- International Hospital Inpatient Quality MeasuresDocument1 pageInternational Hospital Inpatient Quality MeasuresSafiqulatif AbdillahNo ratings yet
- Practice Guidelines For Chronic Pain Management .13Document24 pagesPractice Guidelines For Chronic Pain Management .13Safiqulatif AbdillahNo ratings yet
- NationalguidelinesDocument26 pagesNationalguidelines18saNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Obat YanmedDocument2 pagesObat YanmedSafiqulatif AbdillahNo ratings yet
- Para Lec CombinedDocument83 pagesPara Lec CombinedClent Earl Jason O. BascoNo ratings yet
- Preview: Proquest Dissertations and Theses 2002 Proquest Dissertations & Theses Full TextDocument24 pagesPreview: Proquest Dissertations and Theses 2002 Proquest Dissertations & Theses Full TextFelipe AguilarNo ratings yet
- Practice For Mounting Buses & Joints-374561Document11 pagesPractice For Mounting Buses & Joints-374561a_sengar1No ratings yet
- Orbitol Motor TMTHWDocument20 pagesOrbitol Motor TMTHWRodolfo ErenoNo ratings yet
- Youth Camp Registration Form-2022Document1 pageYouth Camp Registration Form-2022FlerkNo ratings yet
- Kelas ChondrichtyesDocument15 pagesKelas ChondrichtyesanitagustinawatiNo ratings yet
- Principles Involved in Baking 1Document97 pagesPrinciples Involved in Baking 1Milky BoyNo ratings yet
- FactSet London OfficeDocument1 pageFactSet London OfficeDaniyar KaliyevNo ratings yet
- Region 1 - Concreting Works Materials Prices - PHILCON PRICESDocument9 pagesRegion 1 - Concreting Works Materials Prices - PHILCON PRICESMark Gregory RimandoNo ratings yet
- Conceptual Artist in Nigeria UNILAGDocument13 pagesConceptual Artist in Nigeria UNILAGAdelekan FortuneNo ratings yet
- Aquaculture Scoop May IssueDocument20 pagesAquaculture Scoop May IssueAquaculture ScoopNo ratings yet
- Las Tech Drafting 3Q WKDocument13 pagesLas Tech Drafting 3Q WKClemenda TuscanoNo ratings yet
- Goa Daman & Diu Factory Rules PDFDocument141 pagesGoa Daman & Diu Factory Rules PDFmrudang1972100% (1)
- Armadio Presentation-2019Document45 pagesArmadio Presentation-2019Subhash Singh TomarNo ratings yet
- Eco Exercise 3answer Ans 1Document8 pagesEco Exercise 3answer Ans 1Glory PrintingNo ratings yet
- SMAST - 150kW 02190 - 200929091953Document67 pagesSMAST - 150kW 02190 - 200929091953David GarciaNo ratings yet
- Kinder DLL Week 8Document15 pagesKinder DLL Week 8Jainab Pula SaiyadiNo ratings yet
- Ecological Quality RatioDocument24 pagesEcological Quality RatiofoocheehungNo ratings yet
- Rectifier 5G High Density Embedded Power (3U Power Rack, Three Phase Four Wire) E...Document4 pagesRectifier 5G High Density Embedded Power (3U Power Rack, Three Phase Four Wire) E...Lintas LtiNo ratings yet
- Iso 8033 2016Document9 pagesIso 8033 2016Eric ChuNo ratings yet
- Iec60227-3 (Ed2.1) en DDocument6 pagesIec60227-3 (Ed2.1) en Duntuk donlod aaaNo ratings yet
- EXCEL For Pump DesignDocument2 pagesEXCEL For Pump Designkad-7No ratings yet
- Manuscript FsDocument76 pagesManuscript FsRalph HumpaNo ratings yet
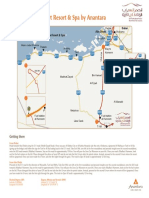
- Qasr Al Sarab Desert Resort Location Map June2012Document1 pageQasr Al Sarab Desert Resort Location Map June2012Anant GârgNo ratings yet
- English2 Q2 Summative Assessment 4 2Document4 pagesEnglish2 Q2 Summative Assessment 4 2ALNIE PANGANIBANNo ratings yet
- The Indian & The SnakeDocument3 pagesThe Indian & The SnakeashvinNo ratings yet
- Javanese PeopleDocument22 pagesJavanese PeopleDenisaNo ratings yet
- Notes Transfer of Thermal EnergyDocument12 pagesNotes Transfer of Thermal Energymahrosh mamoon100% (2)
- 12-Week Off-Season Training Programme Junior Rugby (U18 - U21)Document5 pages12-Week Off-Season Training Programme Junior Rugby (U18 - U21)LeBron JamesNo ratings yet
- 5 Contracting Activity and Technical Staff RequirementsDocument2 pages5 Contracting Activity and Technical Staff RequirementsDaniyar KussainovNo ratings yet