You might also like
- Essential Oils Pocket Reference - Fifth EditionDocument206 pagesEssential Oils Pocket Reference - Fifth Editionbianca7893% (88)
- WellCat Veterinary HandbookDocument36 pagesWellCat Veterinary HandbookKatSiebrecht100% (5)
- Magnetic Resonance Imaging: Recording, Reconstruction and AssessmentFrom EverandMagnetic Resonance Imaging: Recording, Reconstruction and AssessmentRating: 5 out of 5 stars5/5 (1)
- EpilepsyDocument38 pagesEpilepsyJareena BegumNo ratings yet
- A Novel Breast Tumor Classification Algorithm Using Neutrosophic Score FeaturesDocument11 pagesA Novel Breast Tumor Classification Algorithm Using Neutrosophic Score FeaturesMia AmaliaNo ratings yet
- Girl InterruptedDocument7 pagesGirl Interruptedapi-365678992No ratings yet
- Lipo LaserDocument13 pagesLipo LaserLuis A Gil Pantoja100% (1)
- Basic Surgical Skills FinalDocument62 pagesBasic Surgical Skills Finalamel015No ratings yet
- Modifiers-Table 122015 2Document25 pagesModifiers-Table 122015 2khatNo ratings yet
- Full Download Winninghams Critical Thinking Cases in Nursing 5th Edition Harding Solutions ManualDocument28 pagesFull Download Winninghams Critical Thinking Cases in Nursing 5th Edition Harding Solutions Manualnoahmya6100% (25)
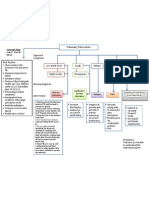
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Diabetic Nephropathy BaruDocument24 pagesDiabetic Nephropathy BaruRobiyanti Nur Chalifah HattaNo ratings yet
- Drug Study - MidazolamDocument2 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- Image Features of True Positive and False Negative Cancers in Screening MammogramsDocument9 pagesImage Features of True Positive and False Negative Cancers in Screening MammogramsTher RayNo ratings yet
- Automated Chest Screening Based On A Hybrid Model of Transfer Learning and Convolutional Sparse Denoising AutoencoderDocument19 pagesAutomated Chest Screening Based On A Hybrid Model of Transfer Learning and Convolutional Sparse Denoising AutoencoderAlejandro De Jesus Romo RosalesNo ratings yet
- Curroncol 29 00159 v2Document20 pagesCurroncol 29 00159 v2rachid oumouloudNo ratings yet
- Birads Score For Mammographic Images: Parveen Jaseela Regina .O. MDocument8 pagesBirads Score For Mammographic Images: Parveen Jaseela Regina .O. MInternational Journal of computational Engineering research (IJCER)No ratings yet
- A Computer-Aided Detection of The Architectural Distortion in Digital Mammograms Using The Fractal Dimension Measurements of BEMD PDFDocument17 pagesA Computer-Aided Detection of The Architectural Distortion in Digital Mammograms Using The Fractal Dimension Measurements of BEMD PDFDanisbNo ratings yet
- Image Classification Approach For Breast Cancer Detection Based On A Complex Event ProcessingDocument8 pagesImage Classification Approach For Breast Cancer Detection Based On A Complex Event ProcessingIOSRJEN : hard copy, certificates, Call for Papers 2013, publishing of journalNo ratings yet
- Thesis On Mammogram ClassificationDocument4 pagesThesis On Mammogram Classificationdwhkp7x5100% (2)
- Keywords Mammogram Adaptive Median Filter GMM Segmentation HMRF-EM GLCMDocument13 pagesKeywords Mammogram Adaptive Median Filter GMM Segmentation HMRF-EM GLCMChamar AshishNo ratings yet
- Breast Cancer Diagnosis in Two-View Mammography Using End-To-End Trained Efficientnet-Based Convolutional NetworkDocument15 pagesBreast Cancer Diagnosis in Two-View Mammography Using End-To-End Trained Efficientnet-Based Convolutional NetworkHuy DuongNo ratings yet
- A Survey of Image Processing Techniques For Detection of MassDocument6 pagesA Survey of Image Processing Techniques For Detection of MassInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Performance Evaluation of Image Processing Algorithms in CadeDocument14 pagesPerformance Evaluation of Image Processing Algorithms in CadePAUL AKAMPURIRANo ratings yet
- Automatic Breast Cancer Detection With Optimized Ensemble of ClassifiersDocument11 pagesAutomatic Breast Cancer Detection With Optimized Ensemble of ClassifiersIAEME PublicationNo ratings yet
- Modeling Human Eye Behavior During Mammographic Scanning: Preliminary ResultsDocument12 pagesModeling Human Eye Behavior During Mammographic Scanning: Preliminary ResultsCHARANNo ratings yet
- Potential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsDocument11 pagesPotential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsMR Emam - GamingNo ratings yet
- Geographical Distribution of Breast Cancers On The Mammogram: An Interval Cancer DatabaseDocument6 pagesGeographical Distribution of Breast Cancers On The Mammogram: An Interval Cancer DatabaseTher RayNo ratings yet
- Evaluation of Doses and Image Quality in Mammography With SF, CR, and DR DetectorsDocument6 pagesEvaluation of Doses and Image Quality in Mammography With SF, CR, and DR DetectorsFrancisco AnastacioNo ratings yet
- Zernike CBM 2011Document10 pagesZernike CBM 2011Jyotsna SinghNo ratings yet
- Breast Cancer Screening Using Convolutional NeuralDocument13 pagesBreast Cancer Screening Using Convolutional NeuralAkash BSDKNo ratings yet
- Breast Cancer Research Paper DipDocument12 pagesBreast Cancer Research Paper DipSuraj KumarNo ratings yet
- 1.principles of ContrastDocument8 pages1.principles of Contrastvidi87No ratings yet
- Journal of Biomedical Informatics: J. Dheeba, N. Albert Singh, S. Tamil SelviDocument8 pagesJournal of Biomedical Informatics: J. Dheeba, N. Albert Singh, S. Tamil SelviAhmed Allah Abd Al ZaherNo ratings yet
- Breast Cancer ScopusDocument5 pagesBreast Cancer ScopusMurat CanNo ratings yet
- IJCER (WWW - Ijceronline.com) International Journal of Computational Engineering ResearchDocument6 pagesIJCER (WWW - Ijceronline.com) International Journal of Computational Engineering ResearchInternational Journal of computational Engineering research (IJCER)No ratings yet
- ConferanceDocument4 pagesConferanceFatihUniversitesi SummerSchoolNo ratings yet
- Breast Invasive Ductal Carcinoma Diagnosis Using Machine Learning Models and Gabor Filter Method of Histology ImagesDocument10 pagesBreast Invasive Ductal Carcinoma Diagnosis Using Machine Learning Models and Gabor Filter Method of Histology ImagesIJRES teamNo ratings yet
- Surgery Using Raman Spectroscopy (?Q1: Running Head: Margin Assessment During Partial Mastectomy BreastDocument7 pagesSurgery Using Raman Spectroscopy (?Q1: Running Head: Margin Assessment During Partial Mastectomy BreastJoan Joel Cáceres RamirezNo ratings yet
- Classification of Breast Cancer Histopathological Images Using Discriminative Patches Screened by Generative Adversarial NetworksDocument16 pagesClassification of Breast Cancer Histopathological Images Using Discriminative Patches Screened by Generative Adversarial NetworksGuru VelmathiNo ratings yet
- Pitcher 2017Document6 pagesPitcher 2017anhca4519No ratings yet
- Skin Lesion Classification From Dermoscopy and Clinical Images With A Deep Learning ApproachDocument7 pagesSkin Lesion Classification From Dermoscopy and Clinical Images With A Deep Learning ApproachIJAR JOURNALNo ratings yet
- An Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesDocument4 pagesAn Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesEditor IJRITCCNo ratings yet
- Fnaqch 94Document26 pagesFnaqch 94Gilberto MartinezNo ratings yet
- Characterizing Architectural Distortion in Mammograms by Linear SaliencyDocument12 pagesCharacterizing Architectural Distortion in Mammograms by Linear SaliencySebastianNo ratings yet
- An Advanced Breast Tumor Classification Algorithm: Dinesh Kumar, Vijay Kumar, Jyoti, Sumer Poonia, Felix Deepak MinjDocument9 pagesAn Advanced Breast Tumor Classification Algorithm: Dinesh Kumar, Vijay Kumar, Jyoti, Sumer Poonia, Felix Deepak MinjGoh DodyNo ratings yet
- IJCTA 1474624942 VenkateshDocument15 pagesIJCTA 1474624942 Venkateshsabby13No ratings yet
- Artificial Neural Network For Cervical Abnormalities Detection On Computed Tomography ImagesDocument9 pagesArtificial Neural Network For Cervical Abnormalities Detection On Computed Tomography ImagesIAES IJAINo ratings yet
- Art 3Document15 pagesArt 3Daniela NaipeanuNo ratings yet
- IJREATV1I1103Document7 pagesIJREATV1I1103Sasi KalaNo ratings yet
- PIIS258975002200070XDocument13 pagesPIIS258975002200070XAnonymous HUY0yRexYfNo ratings yet
- Inbreast PDFDocument13 pagesInbreast PDFPriyanka DattaNo ratings yet
- Inteligencia Artificial: José Daniel López-Cabrera, Luis Alberto López Rodríguez, Marlén Pérez-DíazDocument11 pagesInteligencia Artificial: José Daniel López-Cabrera, Luis Alberto López Rodríguez, Marlén Pérez-DíazSebastian Vallejo RangelNo ratings yet
- Research ProposalDocument10 pagesResearch ProposalyassineNo ratings yet
- Full Field Digital Mammography 2Document27 pagesFull Field Digital Mammography 2CTAFDocumentsNo ratings yet
- Akay 2009Document8 pagesAkay 2009VivekNo ratings yet
- Breast Cancer Screening Modalities, Recommendations, and Novel Imaging TechniquesDocument20 pagesBreast Cancer Screening Modalities, Recommendations, and Novel Imaging TechniquesZuriNo ratings yet
- Inbreast:: Technical ReportDocument13 pagesInbreast:: Technical ReportAli NawazNo ratings yet
- Journal Pone 0269931Document13 pagesJournal Pone 0269931Abdelali MoufidiNo ratings yet
- Breast Cancer LPPDocument9 pagesBreast Cancer LPPrupaj_n954No ratings yet
- Final Paper - DBCDocument6 pagesFinal Paper - DBCsangeerthana sanaNo ratings yet
- Biomolecules 10 01123 v2Document13 pagesBiomolecules 10 01123 v2Adru von MatterhornNo ratings yet
- Breast Cancer Classification From Histopathological Images Using Resolution Adaptive NetworkDocument15 pagesBreast Cancer Classification From Histopathological Images Using Resolution Adaptive NetworkKeren Evangeline. INo ratings yet
- Automated Breast Cancer Detection Using Machine Learning Techniques by Extracting Different Feature Extracting StrategiesDocument5 pagesAutomated Breast Cancer Detection Using Machine Learning Techniques by Extracting Different Feature Extracting Strategiesmanoj523No ratings yet
- A Representation For Mammographic Image Processing: Ralph Highnam, Michael Brady and Basil ShepstoneDocument18 pagesA Representation For Mammographic Image Processing: Ralph Highnam, Michael Brady and Basil ShepstoneMario SansoneNo ratings yet
- Bi Rads AnalisisDocument44 pagesBi Rads AnalisisDiego SánchezNo ratings yet
- KJR 17 59Document10 pagesKJR 17 59Regi FauzanNo ratings yet
- Эластография 1Document8 pagesЭластография 1Роман КлоковNo ratings yet
- Application of Fractal Analysis To MammographyDocument4 pagesApplication of Fractal Analysis To MammographyMarco Jimenez HerreraNo ratings yet
- Contrast-Enhanced MammographyFrom EverandContrast-Enhanced MammographyMarc LobbesNo ratings yet
- Parameters of The Model: Name Live Alpha Beta DescriptionDocument5 pagesParameters of The Model: Name Live Alpha Beta DescriptionAngga Prawira KautsarNo ratings yet
- Incision SitesDocument4 pagesIncision SitesmidskiescreamzNo ratings yet
- Endodontics Pain Control in Endodontics: Differential Diagnosis of Dental PainDocument4 pagesEndodontics Pain Control in Endodontics: Differential Diagnosis of Dental Painريام الموسويNo ratings yet
- DKA Handout1Document59 pagesDKA Handout1aleNo ratings yet
- NCPDocument2 pagesNCPfierfizNo ratings yet
- An Unconscious Patient With A DNR TattooDocument2 pagesAn Unconscious Patient With A DNR TattoonadaNo ratings yet
- Raynaud's DiseaseDocument8 pagesRaynaud's DiseaseAhmad Barrun NidhomNo ratings yet
- Student Excursion Consent FormDocument4 pagesStudent Excursion Consent Formapi-276186998No ratings yet
- Etamsylate DS Meppo2010 PDFDocument3 pagesEtamsylate DS Meppo2010 PDFAqmarlia PutriNo ratings yet
- Grand Case Presentation InformationDocument7 pagesGrand Case Presentation InformationCristina L. JaysonNo ratings yet
- P1 RleDocument34 pagesP1 RleMary Jean GicaNo ratings yet
- Carotid Sinus Massage - MuraliDocument31 pagesCarotid Sinus Massage - MuraliAhsan MohammedNo ratings yet
- CH 14 Antepartum Nursing Assessment NotesDocument8 pagesCH 14 Antepartum Nursing Assessment NotesMary LowryNo ratings yet
- Data 14-12-2021 Formulir TB TerbaruDocument1 pageData 14-12-2021 Formulir TB TerbaruAksaNo ratings yet
- CBDRP Reporting Form 1Document1 pageCBDRP Reporting Form 1Romer EnajeNo ratings yet
- Comorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Document10 pagesComorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dini AgustiniNo ratings yet
- WEVM Chapter 1Document22 pagesWEVM Chapter 1Manoj KarkiNo ratings yet
- Avian Influenza in ChickensDocument19 pagesAvian Influenza in ChickensShah NawazNo ratings yet
- WES Ablasi SVT AVRT - Travilla Bastian A. PangestutiDocument1 pageWES Ablasi SVT AVRT - Travilla Bastian A. PangestutiHervin RamadhaniNo ratings yet