You might also like
- Anatomy of Human Skull and BonesDocument25 pagesAnatomy of Human Skull and BonesJohnvee Magana100% (2)
- Stiinta WaldorfDocument274 pagesStiinta Waldorfarchie100% (1)
- Thyroid Disease in PregnancyDocument12 pagesThyroid Disease in PregnancyOldriana Prawiro HapsariNo ratings yet
- Development of The Face, Oral Cavity & Pharyngeal Arches - PILLAYDocument48 pagesDevelopment of The Face, Oral Cavity & Pharyngeal Arches - PILLAYOHupdatesNo ratings yet
- Thyroid Disease in PregnancyDocument70 pagesThyroid Disease in PregnancyRajeev Sood100% (1)
- Acog Practice Bulletin TiroidesDocument10 pagesAcog Practice Bulletin TiroidesMerpi Alvarez Goris100% (1)
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocument36 pagesThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNo ratings yet
- Face Massage PDFDocument6 pagesFace Massage PDFLakshita PrajapatiNo ratings yet
- 148 Thyroid Disease in PregnancyDocument10 pages148 Thyroid Disease in Pregnancyobgin uiNo ratings yet
- A Hierarchical Model For Evaluation and Treatment of Visual Perceptual Dysfunction in Adult Acquired Brain Injury Part 1Document13 pagesA Hierarchical Model For Evaluation and Treatment of Visual Perceptual Dysfunction in Adult Acquired Brain Injury Part 1Sebastian CheungNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Thyroid Disease in PregnancyDocument24 pagesThyroid Disease in PregnancyKai XinNo ratings yet
- 14-Oral CavityDocument36 pages14-Oral CavitykavindukarunarathnaNo ratings yet
- Patient's medical data reportDocument32 pagesPatient's medical data reportraman kumariNo ratings yet
- Anatomy & Physiology of Olfactory System.Document27 pagesAnatomy & Physiology of Olfactory System.Prasanna DattaNo ratings yet
- TiroidopatiasDocument10 pagesTiroidopatiasArantza PelaezNo ratings yet
- Enfermedad Tiroides y Embarazo ACOGDocument10 pagesEnfermedad Tiroides y Embarazo ACOGDairo PintoNo ratings yet
- TiroideDocument10 pagesTiroideRosália CoutadaNo ratings yet
- Enfermedades Tiroideas en El EmbarazoDocument14 pagesEnfermedades Tiroideas en El EmbarazoMelissa Gómez CruzNo ratings yet
- Screenshot 2022-10-07 at 5.51.47 AMDocument14 pagesScreenshot 2022-10-07 at 5.51.47 AMManuel PuertaNo ratings yet
- Cme Reviewarticle: Diagnosis and Management of Hyperthyroidism in Pregnancy: A ReviewDocument11 pagesCme Reviewarticle: Diagnosis and Management of Hyperthyroidism in Pregnancy: A ReviewErnestNo ratings yet
- Hyperthyroidism PregnancyDocument3 pagesHyperthyroidism PregnancySyahfiq IsmailNo ratings yet
- Tiroid Disease 14 HalamanDocument14 pagesTiroid Disease 14 HalamanDevi SuryandariNo ratings yet
- Thyroid Dysfunction During Pregnancy: A Review of The Current GuidelinesDocument7 pagesThyroid Dysfunction During Pregnancy: A Review of The Current GuidelinesSSR-IIJLS JournalNo ratings yet
- Grave DiseaseDocument6 pagesGrave DiseaseFakrocev Charlie GuloNo ratings yet
- Hyperthyroidism in Pregnancy: Jorge H. MDDocument23 pagesHyperthyroidism in Pregnancy: Jorge H. MDRashid HussainNo ratings yet
- Thyroid Disease in Pregnancy v3.6Document9 pagesThyroid Disease in Pregnancy v3.6nino.matasNo ratings yet
- Akibat Pada Kehamilan Akibat Pada KehamilanDocument4 pagesAkibat Pada Kehamilan Akibat Pada KehamilanTrisnawanta Asih PasamboNo ratings yet
- Thyroid Physiology and Common Diseases in Pregnancy: Review of LiteratureDocument8 pagesThyroid Physiology and Common Diseases in Pregnancy: Review of LiteratureMarijeimy Alejandra Ortíz FerroNo ratings yet
- Thyroid Disorders in PregnancyDocument3 pagesThyroid Disorders in PregnancyZoel Nikonian100% (1)
- Therapeutic Approach of Fetal Thyroid Disorders: Research inDocument5 pagesTherapeutic Approach of Fetal Thyroid Disorders: Research inAlma Veronica Gonzalez SandovalNo ratings yet
- Good Clinical Practice Advice: Thyroid and PregnancyDocument5 pagesGood Clinical Practice Advice: Thyroid and Pregnancyjuan carlos pradaNo ratings yet
- Thyroid Disorders During Pregnancy and A PDFDocument6 pagesThyroid Disorders During Pregnancy and A PDFtania jannah100% (1)
- Hyperthyroidism in Pregnancy: Management GuidelinesDocument22 pagesHyperthyroidism in Pregnancy: Management GuidelinesRashid HussainNo ratings yet
- Pregnancy Thyroid DiseaseDocument8 pagesPregnancy Thyroid DiseaseYhang Lidi TamaNo ratings yet
- Hypothyroidism and Pregnancy Vol.2Document9 pagesHypothyroidism and Pregnancy Vol.2RakhiNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument7 pagesJournal of Clinical & Translational EndocrinologyCindyTariganNo ratings yet
- Bioscientific Review (BSR)Document10 pagesBioscientific Review (BSR)UMT JournalsNo ratings yet
- Managing Thyroid Storm in a Pregnant PatientDocument10 pagesManaging Thyroid Storm in a Pregnant PatientAulia CahyaniNo ratings yet
- Jurnal Hipertiroid KehamilanDocument5 pagesJurnal Hipertiroid KehamilanAbdurrohman IzzuddinNo ratings yet
- Эндокринологическая патология и беременность 2018Document50 pagesЭндокринологическая патология и беременность 2018Med PoxNo ratings yet
- Tiroid Pada KehamilanDocument56 pagesTiroid Pada Kehamilanpeni_dwi100% (1)
- Hypertiroid PD KehamilanDocument7 pagesHypertiroid PD KehamilanAD MonikaNo ratings yet
- Emergencias EndocrinasDocument6 pagesEmergencias EndocrinasAlex Andrés Cuevas UrriolaNo ratings yet
- Gestational Transient Thyrotoxicosis: M. Taha Albaar, John MF AdamDocument6 pagesGestational Transient Thyrotoxicosis: M. Taha Albaar, John MF AdamMaulana Rahmat HidayatullahNo ratings yet
- Preconception Counseling For Thyroid DisordersDocument7 pagesPreconception Counseling For Thyroid DisordersLiya AnjelinaNo ratings yet
- Hypothyroidism and Hyperthyroidism in Pregnancy: Mafauzy MohamedDocument25 pagesHypothyroidism and Hyperthyroidism in Pregnancy: Mafauzy MohamedFatima ZahraNo ratings yet
- [1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancyDocument8 pages[1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancyClaudia IrimieNo ratings yet
- Assessment and Treatment of Thyroid Disorders in Pregnancy and The Postpartum PeriodDocument14 pagesAssessment and Treatment of Thyroid Disorders in Pregnancy and The Postpartum PeriodErick HernandezNo ratings yet
- Thyroid Storm Diagnosis and Treatment ChallengesDocument7 pagesThyroid Storm Diagnosis and Treatment ChallengesKarl Angelo MontanoNo ratings yet
- Endocrine Pathology Associated With Pregnancy Dr. Yunus TanggoDocument60 pagesEndocrine Pathology Associated With Pregnancy Dr. Yunus TanggoReni AstutiNo ratings yet
- Hipotiroidism Diaz 2014Document17 pagesHipotiroidism Diaz 2014Achmad ArrizalNo ratings yet
- Management of Babies Born to Mothers with Thyroid DiseaseDocument5 pagesManagement of Babies Born to Mothers with Thyroid DiseasexanderaleNo ratings yet
- Management and follow-up of thyroid cancer in pregnant womenDocument8 pagesManagement and follow-up of thyroid cancer in pregnant womenMiguel EspinosaNo ratings yet
- Comparison of The American Thyroid Association With The Endocrine Society Practice Guidelines For The Screening and Treatment of Hypothyroidism During PregnancyDocument7 pagesComparison of The American Thyroid Association With The Endocrine Society Practice Guidelines For The Screening and Treatment of Hypothyroidism During PregnancySus ArNo ratings yet
- Thyroid Function in Pre EcclampsiaDocument3 pagesThyroid Function in Pre EcclampsiaIOSRjournalNo ratings yet
- Pregnancy with HyperthyroidismDocument2 pagesPregnancy with HyperthyroidismAnonymous XOE26kbtvdNo ratings yet
- Thyroid Disease in Pregnancy: New Insights in Diagnosis and Clinical ManagementDocument14 pagesThyroid Disease in Pregnancy: New Insights in Diagnosis and Clinical ManagementBTS LGONo ratings yet
- ThyroidDocument16 pagesThyroidnawaNo ratings yet
- Medicine Pearls on HypothyroidismDocument5 pagesMedicine Pearls on Hypothyroidismlegend789No ratings yet
- GD in PregnancyDocument37 pagesGD in Pregnancymohammed makkiNo ratings yet
- Thyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesDocument8 pagesThyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesLolla MorsiNo ratings yet
- Neonatal Hyperthyroidism: Screening and ManagementDocument10 pagesNeonatal Hyperthyroidism: Screening and ManagementAzucena HernandezNo ratings yet
- Pregnancy Thyroid Disease 508Document12 pagesPregnancy Thyroid Disease 508Ankush RanaNo ratings yet
- Prevalence of Subclinical and Undiagnosed Overt Hypothyroidismin Habitual AbortionDocument7 pagesPrevalence of Subclinical and Undiagnosed Overt Hypothyroidismin Habitual AbortionIJAR JOURNALNo ratings yet
- Development of the Musical BrainDocument18 pagesDevelopment of the Musical BrainLeyla Da Silva AugustoNo ratings yet
- Brain Encephalon: - Brain: Embrionally Comes From Ectoderm PartDocument72 pagesBrain Encephalon: - Brain: Embrionally Comes From Ectoderm PartHana AdivaNo ratings yet
- Anatomy and Physiology II Test 1 Review: Special Senses, Ears, EndocrineDocument5 pagesAnatomy and Physiology II Test 1 Review: Special Senses, Ears, EndocrineMichelle BacaNo ratings yet
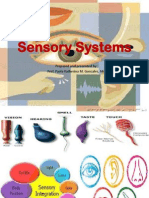
- Sensory Systems OverviewDocument72 pagesSensory Systems OverviewcholoNo ratings yet
- H&N Mod. Wk1 ScalpDocument10 pagesH&N Mod. Wk1 ScalpUloko ChristopherNo ratings yet
- History of Present IllnessDocument70 pagesHistory of Present IllnessKlb ElbnatNo ratings yet
- Juvenile Nasopharyngeal Angiofibroma SurgeryDocument18 pagesJuvenile Nasopharyngeal Angiofibroma Surgeryarief ardaNo ratings yet
- 6 Q1-PerDev - ForstudentsDocument16 pages6 Q1-PerDev - ForstudentsBoyet CatalanNo ratings yet
- Imaging of The Ear - X Ray of The Temporal Bone, Schuller's ProjectionDocument25 pagesImaging of The Ear - X Ray of The Temporal Bone, Schuller's ProjectionHisbulloh syarifNo ratings yet
- Maxillary Reconstruction: By: Anteneh Gebru (MD, PSR 4, Aau, Alert Center)Document40 pagesMaxillary Reconstruction: By: Anteneh Gebru (MD, PSR 4, Aau, Alert Center)Anteneh GebruNo ratings yet
- Laboratory Services: Patient Name Lab No Uhid Sample Date Age/Gender Receiving Date Referred by Report Date Report StatusDocument26 pagesLaboratory Services: Patient Name Lab No Uhid Sample Date Age/Gender Receiving Date Referred by Report Date Report StatusTamzid Rabby TanmoyNo ratings yet
- H & N - Pharynx& Deglutition PDFDocument17 pagesH & N - Pharynx& Deglutition PDFRamin AmirkhiziNo ratings yet
- Nervous system essentialsDocument10 pagesNervous system essentialsLeboNo ratings yet
- Crop Fade Haircut Fade - Google AramaDocument1 pageCrop Fade Haircut Fade - Google Aramafatih yiğitNo ratings yet
- "Water On The Brain": Types of HydrocephalusDocument2 pages"Water On The Brain": Types of Hydrocephalusbea pegadNo ratings yet
- Anatomy and Physiology Tetanus FinalDocument17 pagesAnatomy and Physiology Tetanus Finalfelicisimo039690175% (4)
- Dysphagia NotesDocument5 pagesDysphagia Notesapi-31372205650% (2)
- Wear It Right (3M)Document2 pagesWear It Right (3M)wfng77No ratings yet
- Tapsa THE EARDocument4 pagesTapsa THE EARgalileeNo ratings yet
- OAP 2010 Practical 1 - Anatomy of Eye and AppendagesDocument14 pagesOAP 2010 Practical 1 - Anatomy of Eye and Appendagesslawren11No ratings yet
- Nervous and Endocrine System: Marc Andreo C. Malala, RN, MANDocument18 pagesNervous and Endocrine System: Marc Andreo C. Malala, RN, MANMarc Andreo MalalaNo ratings yet
- Radiographic Classification of Temporal Bone Fractures: Clinical Predictability Using A New SystemDocument5 pagesRadiographic Classification of Temporal Bone Fractures: Clinical Predictability Using A New SystemTaufik ShidkiNo ratings yet

















































![[1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancy](https://imgv2-1-f.scribdassets.com/img/document/552054434/149x198/0ad7f435ea/1710545307?v=1)