You might also like
- Bone Marrow Edema SyndromeDocument12 pagesBone Marrow Edema SyndromearuggeriNo ratings yet
- A Systematic Review of Outcomes and Complications of Treating Unstable Distal Radius Fractures in The Elderly PDFDocument26 pagesA Systematic Review of Outcomes and Complications of Treating Unstable Distal Radius Fractures in The Elderly PDFaruggeriNo ratings yet
- A Brief Overview and Update of Myofascial Pain Syndrome and Myofascial Trigger Points PDFDocument10 pagesA Brief Overview and Update of Myofascial Pain Syndrome and Myofascial Trigger Points PDFaruggeriNo ratings yet
- Illness Behavior in Patients On Long-Term Sick Leave Due To Chronic Musculoskeletal PainDocument6 pagesIllness Behavior in Patients On Long-Term Sick Leave Due To Chronic Musculoskeletal PainaruggeriNo ratings yet
- Coronoid Fractures of The ElbowDocument5 pagesCoronoid Fractures of The ElbowaruggeriNo ratings yet
- Effect of Wrist Joint Restriction On Forearm and Shoulder Movement During Upper Extremity Functional ActivitiesDocument4 pagesEffect of Wrist Joint Restriction On Forearm and Shoulder Movement During Upper Extremity Functional ActivitiesaruggeriNo ratings yet
- Evaluation of Cervical Proprioceptive Function PDFDocument10 pagesEvaluation of Cervical Proprioceptive Function PDFaruggeriNo ratings yet
- Measurement of Pectoralis Minor Muscle Length - Validation and Clinical ApplicationDocument7 pagesMeasurement of Pectoralis Minor Muscle Length - Validation and Clinical ApplicationaruggeriNo ratings yet
- A Systematic Review and Meta-Analysis of Clinical Trials On Physical Interventions For Lateral EpicondylalgiaDocument12 pagesA Systematic Review and Meta-Analysis of Clinical Trials On Physical Interventions For Lateral EpicondylalgiaaruggeriNo ratings yet
- Biceps Load Test II. A Clinical Test For SLAP LesionsDocument5 pagesBiceps Load Test II. A Clinical Test For SLAP LesionsaruggeriNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Relative ClausesDocument7 pagesRelative ClausesEvaluna MoidalNo ratings yet
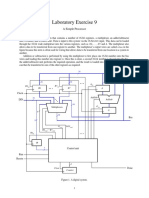
- Laboratory Exercise 9: A Simple ProcessorDocument8 pagesLaboratory Exercise 9: A Simple ProcessorhxchNo ratings yet
- Emergency procedures for shipboard fire suppression systemsDocument1 pageEmergency procedures for shipboard fire suppression systemsImmorthalNo ratings yet
- Week 1 - Topic: Chapter 2: The Foreign Exchange Market 21 March 2021Document36 pagesWeek 1 - Topic: Chapter 2: The Foreign Exchange Market 21 March 2021Jenita singhNo ratings yet
- Thursday Forenoon: Instant Examinations - June - 2018Document6 pagesThursday Forenoon: Instant Examinations - June - 2018Gurusamy GuruNo ratings yet
- 2023 Imec Wind Symphony ProgramDocument16 pages2023 Imec Wind Symphony Programapi-583612673No ratings yet
- Is 2572 (2005) - Construction of Hollow and Solid Concrete Block Masonry - Code of PracticeDocument27 pagesIs 2572 (2005) - Construction of Hollow and Solid Concrete Block Masonry - Code of PracticeVIDYANo ratings yet
- Civil TechnologyDocument2 pagesCivil TechnologyLeonicia MarquinezNo ratings yet
- Pushover Analysis As Per EC8Document23 pagesPushover Analysis As Per EC8mihaitimofteNo ratings yet
- Reliability Centered Maintenance ExplainationDocument6 pagesReliability Centered Maintenance Explainationambuenaflor100% (1)
- S.Y. Resistance of A Galvanometer G by Shunting GR - IIDocument2 pagesS.Y. Resistance of A Galvanometer G by Shunting GR - IINeelam KapoorNo ratings yet
- BAMBOO PRESERVATION TECHNIQUESDocument36 pagesBAMBOO PRESERVATION TECHNIQUESAianne de VeraNo ratings yet
- Facebook Ads Defeat Florida Ballot InitiativeDocument3 pagesFacebook Ads Defeat Florida Ballot InitiativeGuillermo DelToro JimenezNo ratings yet
- LSE100 Past Year Questions (2014/5)Document2 pagesLSE100 Past Year Questions (2014/5)Jingwen ZhangNo ratings yet
- User's Manual: & Technical DocumentationDocument20 pagesUser's Manual: & Technical DocumentationPODOSALUD HUANCAYONo ratings yet
- Bailey - Butch - Queens - Up - in - Pumps - Gender, - Performance, - and - ... - (Chapter - One. - Introduction - Peforming - Gender, - Creating - Kinship, - Forging - ... )Document28 pagesBailey - Butch - Queens - Up - in - Pumps - Gender, - Performance, - and - ... - (Chapter - One. - Introduction - Peforming - Gender, - Creating - Kinship, - Forging - ... )ben100% (1)
- Power: Definition and TypesDocument3 pagesPower: Definition and TypesShashi RanjanNo ratings yet
- Chaity-Group New ProfileDocument39 pagesChaity-Group New ProfileShajedul PalashNo ratings yet
- Engineering Economics - Solution Manual (Chapter 1)Document1 pageEngineering Economics - Solution Manual (Chapter 1)Diego GuineaNo ratings yet
- The Metabolic and Endocrine Systems NotesDocument9 pagesThe Metabolic and Endocrine Systems NotesCarl Elexer Cuyugan Ano100% (2)
- Materials of Engineering Lecture Unit 1 Pptmaten22Document24 pagesMaterials of Engineering Lecture Unit 1 Pptmaten22Ignacio Flores CaballeroNo ratings yet
- First Masterclass Progress Test 1Document4 pagesFirst Masterclass Progress Test 1Billy Herington fullmasterNo ratings yet
- 8086 Instruction Set and Assembly Language ProgramDocument13 pages8086 Instruction Set and Assembly Language Programwaheed azizNo ratings yet
- ASA-RAC Application GuideDocument15 pagesASA-RAC Application GuideIsrael Miranda Zamarca100% (2)
- NSO Class 6 Sample Paper 2019 20Document3 pagesNSO Class 6 Sample Paper 2019 20NitinNo ratings yet
- The Demands of Society From The Teacher As A PersonDocument2 pagesThe Demands of Society From The Teacher As A PersonKyle Ezra Doman100% (1)
- Multimedia Unit 2Document12 pagesMultimedia Unit 2Shashank SaxenaNo ratings yet
- Default Password For All TMNet Streamyx Supported ModemDocument2 pagesDefault Password For All TMNet Streamyx Supported ModemFrankly F. ChiaNo ratings yet
- DLL - Science 5 - Q3 - W2Document10 pagesDLL - Science 5 - Q3 - W2Eihcra SubacNo ratings yet
- High Pressure Check Valves 150119Document6 pagesHigh Pressure Check Valves 150119Nilesh MistryNo ratings yet