You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Toxic Epidermal Necrolysis: BackgroundDocument36 pagesToxic Epidermal Necrolysis: BackgroundGita AmeliaNo ratings yet
- ReferatDocument3 pagesReferatGita AmeliaNo ratings yet
- ReferatDocument36 pagesReferatGita AmeliaNo ratings yet
- An Unusual Presentation of Multiple Cavitated Lung Metastases From Colon CarcinomaDocument4 pagesAn Unusual Presentation of Multiple Cavitated Lung Metastases From Colon CarcinomaGita AmeliaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Winning DartsDocument182 pagesWinning DartsSameer NandanNo ratings yet
- Wa0001Document1 pageWa0001Boru RajaNo ratings yet
- Transcutaneous Nerve StimulationDocument6 pagesTranscutaneous Nerve StimulationARGNo ratings yet
- Nursing Care Plan Ineffective Airway ClearanceDocument3 pagesNursing Care Plan Ineffective Airway Clearancederic100% (13)
- ... My Reflection On Action (Leadershinp and Management)Document15 pages... My Reflection On Action (Leadershinp and Management)Yasmeen zulfiqarNo ratings yet
- Pain Management and Unani MedicineDocument1 pagePain Management and Unani MedicineMSKCNo ratings yet
- Virginia Workers' Compensation Claim Surgery Approval DisputeDocument10 pagesVirginia Workers' Compensation Claim Surgery Approval Disputedbircs777No ratings yet
- PNLE Reviewer With Rationale 1Document12 pagesPNLE Reviewer With Rationale 1Zyla Malinao100% (1)
- Nursing Care Plan UlcerDocument2 pagesNursing Care Plan Ulcerxrampley2100% (2)
- Acute Abdomen Guide: Causes, Symptoms & ManagementDocument33 pagesAcute Abdomen Guide: Causes, Symptoms & ManagementMohammed FaragNo ratings yet
- NP4 Recalls7Document11 pagesNP4 Recalls7AhrisJeannine EscuadroNo ratings yet
- The Kadoka Press, May 3, 2012Document10 pagesThe Kadoka Press, May 3, 2012surfnewmediaNo ratings yet
- 600 Confusing English Words ExplainedDocument209 pages600 Confusing English Words Explainedata nazariNo ratings yet
- Ultrasound-Guided Supraclavicular Nerve Block Safer and Faster Than Landmark TechniqueDocument5 pagesUltrasound-Guided Supraclavicular Nerve Block Safer and Faster Than Landmark Techniquemir sahirNo ratings yet
- A Study To Assess The Level of Anxiety Among The Oncology Patient Receiving Radiotherapy in Selected Cancer Hospital in BangaloreDocument17 pagesA Study To Assess The Level of Anxiety Among The Oncology Patient Receiving Radiotherapy in Selected Cancer Hospital in BangaloreSri HariNo ratings yet
- Herniated Lumbar Intervertebral DiskDocument10 pagesHerniated Lumbar Intervertebral DiskRoberto López MataNo ratings yet
- Sound Healing PresentationDocument26 pagesSound Healing Presentationtushar100% (4)
- Cervical SpondylosisDocument8 pagesCervical SpondylosisRicha AgarwallaNo ratings yet
- Therapeutic Uses of Pineapple-Extracted Bromelain in Surgical CareDocument5 pagesTherapeutic Uses of Pineapple-Extracted Bromelain in Surgical Carebagas100% (1)
- VAMA Poster2Document1 pageVAMA Poster2CEDIVA DeniaNo ratings yet
- Shawa - Patients Perceptions Regarding Nursing Care in The General Surgical Wards at Kenyatta National Hospital - NinisannnDocument103 pagesShawa - Patients Perceptions Regarding Nursing Care in The General Surgical Wards at Kenyatta National Hospital - Ninisannnnoronisa talusobNo ratings yet
- Nejmcp 2032396Document10 pagesNejmcp 2032396juan carlosNo ratings yet
- Analgesia For Labor and Vaginal DeliveryDocument21 pagesAnalgesia For Labor and Vaginal DeliveryLouije MombzNo ratings yet
- Clinical Rehabilitation: Goal Attainment Scaling (GAS) in Rehabilitation: A Practical GuideDocument12 pagesClinical Rehabilitation: Goal Attainment Scaling (GAS) in Rehabilitation: A Practical GuideMarla Constanza Martinez RoseroNo ratings yet
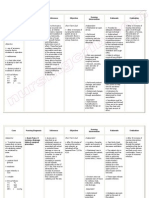
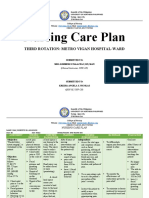
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDocument5 pagesNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasNo ratings yet
- User ManualDocument31 pagesUser ManualJuan Carlos Valverde ValverdeNo ratings yet
- The Effect of The Facilitated Tucking Position in Reducing Vaccination-Induced Pain in NewbornsDocument7 pagesThe Effect of The Facilitated Tucking Position in Reducing Vaccination-Induced Pain in NewbornsCassanovaNovaNo ratings yet
- FK Conox Product Brochure 4ppa4 v6Document4 pagesFK Conox Product Brochure 4ppa4 v6Lucas ShotsNo ratings yet
- Chapter 8. Pain Pathways and Mechanisms of The Pulpodentin Complex - CompressedDocument26 pagesChapter 8. Pain Pathways and Mechanisms of The Pulpodentin Complex - CompressedPaola cruzNo ratings yet
- Cause Effect ParagraphDocument4 pagesCause Effect ParagraphZineb AmelNo ratings yet