You might also like
- Psychology of Women 401 807Document407 pagesPsychology of Women 401 807Alessio TinerviaNo ratings yet
- Nihms 368707Document19 pagesNihms 368707Moh SuprayogiNo ratings yet
- Gender Differences in the Pathogenesis and Management of Heart DiseaseFrom EverandGender Differences in the Pathogenesis and Management of Heart DiseaseNo ratings yet
- Gender Differences in HTN-Doumas Et Al 2013Document10 pagesGender Differences in HTN-Doumas Et Al 2013Bumbum AtaunNo ratings yet
- Epid of Pancreatic CancerDocument2 pagesEpid of Pancreatic CancerHananya ManroeNo ratings yet
- Risk Factors For Cardiovascular Disease in Women: Assessment and ManagementDocument7 pagesRisk Factors For Cardiovascular Disease in Women: Assessment and ManagementAlexandra NiculescuNo ratings yet
- Epidemiology, Risk Factors, and Natural History of Peripheral Artery DiseaseDocument20 pagesEpidemiology, Risk Factors, and Natural History of Peripheral Artery Diseasesnyder120792No ratings yet
- Nej M 199506293322607Document9 pagesNej M 199506293322607Galuh Kresna BayuNo ratings yet
- A Fib 1Document12 pagesA Fib 1palak32No ratings yet
- Leading Causes of Death by Race and Ethnicity in The United States - EditedDocument7 pagesLeading Causes of Death by Race and Ethnicity in The United States - EditedMichael OmolloNo ratings yet
- Gender Differences in Cardiovascular Disease: Short CommunicationDocument3 pagesGender Differences in Cardiovascular Disease: Short CommunicationMoh SuprayogiNo ratings yet
- Literature Review FinalDocument18 pagesLiterature Review Finalapi-458045853No ratings yet
- Risk Factors For Cardiovascular Disease in Women: Assessment and ManagementDocument7 pagesRisk Factors For Cardiovascular Disease in Women: Assessment and ManagementIntania RosatiNo ratings yet
- R245 FullDocument11 pagesR245 FullYuliana WiralestariNo ratings yet
- Cardio Part4.4Document6 pagesCardio Part4.4Jisel-Apple BulanNo ratings yet
- NCDs 2Document100 pagesNCDs 2Fauziyah Farah RNo ratings yet
- Understanding The Complexity of Heart Failure Risk and Treatment in Black PatientsDocument2 pagesUnderstanding The Complexity of Heart Failure Risk and Treatment in Black PatientsRAFNo ratings yet
- United States StatisticsDocument1 pageUnited States StatisticsMohammadAwitNo ratings yet
- 2011 Cardiovascular Disease Prevention in WomenDocument20 pages2011 Cardiovascular Disease Prevention in WomenRafi UllahNo ratings yet
- SP 4: Systemic Lupus Erythematosus: Bagus Suryana Aditya 1670121061 SGD 8 Semester VIDocument12 pagesSP 4: Systemic Lupus Erythematosus: Bagus Suryana Aditya 1670121061 SGD 8 Semester VISuryana AdityaNo ratings yet
- Eur Heart J Suppl 2010 Tardif C2 C10Document9 pagesEur Heart J Suppl 2010 Tardif C2 C10Patrick AlingNo ratings yet
- Downing p2d1 CamDocument7 pagesDowning p2d1 Camapi-384457748No ratings yet
- Key Messages and FactsDocument7 pagesKey Messages and FactsClickon DetroitNo ratings yet
- Ni Hms 366201Document17 pagesNi Hms 366201Habiburrahman EffendyNo ratings yet
- Cardiovascular Risk in Women: Focus On Hypertension: ReviewDocument7 pagesCardiovascular Risk in Women: Focus On Hypertension: ReviewStefane OliveiraNo ratings yet
- Appelman - Sex Differences in Cardiovascular Risk Factors - 2015Document8 pagesAppelman - Sex Differences in Cardiovascular Risk Factors - 2015MIRIAM VIDURRIZAGANo ratings yet
- Why Do Black Americans Have Higher Prevalence of Hypertension?Document2 pagesWhy Do Black Americans Have Higher Prevalence of Hypertension?Christ TopelNo ratings yet
- Week 2 Written AssignmentDocument3 pagesWeek 2 Written Assignmentapi-361631973No ratings yet
- Torre 2015Document19 pagesTorre 2015jenny12No ratings yet
- Women Health IssuesDocument14 pagesWomen Health IssuesAhmadNo ratings yet
- Commentary Hypertension in Men: Phyllis AugustDocument4 pagesCommentary Hypertension in Men: Phyllis AugustDeriven TewengNo ratings yet
- Women Health IssuesDocument14 pagesWomen Health IssuesAhmadNo ratings yet
- Womenshealth & NutritionDocument5 pagesWomenshealth & Nutritionbragaru.vladNo ratings yet
- Journal About Stroke (Pat)Document4 pagesJournal About Stroke (Pat)Patricia Kaye Tayag CastroNo ratings yet
- Adi Id EvDocument21 pagesAdi Id EvKumar AdityaNo ratings yet
- Final Group Project Report: "Hypertension in California"Document8 pagesFinal Group Project Report: "Hypertension in California"May Corpuz100% (1)
- Mortality in Non-Insulin-Dependent Diabetes: Linda S. Geiss, Ma William H. Herman, MD, MPH and Philip J. Smith, PHDDocument26 pagesMortality in Non-Insulin-Dependent Diabetes: Linda S. Geiss, Ma William H. Herman, MD, MPH and Philip J. Smith, PHDblueiceNo ratings yet
- Journal Review PDFDocument5 pagesJournal Review PDFGABRIELLE DE LEONNo ratings yet
- Week 2 Writing AssisgnmentDocument5 pagesWeek 2 Writing Assisgnmentapi-322388539No ratings yet
- CVD Prevalence, Risk, and PathophysiologyDocument79 pagesCVD Prevalence, Risk, and PathophysiologyRani Oktaviani SidaurukNo ratings yet
- The Silent Epidemic of Male Suicide: Dan Bilsker, PHD, Jennifer White, EddDocument6 pagesThe Silent Epidemic of Male Suicide: Dan Bilsker, PHD, Jennifer White, EddincaudasemperNo ratings yet
- Likelihood That A Woman Will Have No Major Risk Factors at The Time of First Myocardial Infarction or StrokeDocument4 pagesLikelihood That A Woman Will Have No Major Risk Factors at The Time of First Myocardial Infarction or StrokeElizar JarNo ratings yet
- Epidemiology of Coronary Heart Disease and Acute Coronary SyndromeDocument6 pagesEpidemiology of Coronary Heart Disease and Acute Coronary SyndromeAnonymous GpgioaDAbNo ratings yet
- Colorectal Cancer Epidemiology: Incidence, Mortality, Survival, and Risk FactorsDocument7 pagesColorectal Cancer Epidemiology: Incidence, Mortality, Survival, and Risk FactorsCamy CarmenNo ratings yet
- Rising Morbidity and Mortality in Midlife Among White Non-Hispanic Americans in The 21st CenturyDocument6 pagesRising Morbidity and Mortality in Midlife Among White Non-Hispanic Americans in The 21st CenturysignalhucksterNo ratings yet
- China-Updated PDFDocument6 pagesChina-Updated PDFCeline Kyla MalloNo ratings yet
- More Colon Cancer Cases Found in Younger People, New Report ShowDocument4 pagesMore Colon Cancer Cases Found in Younger People, New Report ShowEkkoNo ratings yet
- Holy Spirit Hospital PortfolioDocument4 pagesHoly Spirit Hospital Portfolioapi-326916153No ratings yet
- Gender Differences in Ischemic Heart Disease: Ryotaro Wake and Minoru YoshiyamaDocument7 pagesGender Differences in Ischemic Heart Disease: Ryotaro Wake and Minoru YoshiyamaChirag ParmarNo ratings yet
- An HIV Epidemic?Document4 pagesAn HIV Epidemic?The Council of State GovernmentsNo ratings yet
- Women and Heart DiseaseDocument31 pagesWomen and Heart DiseasesuperherosavesNo ratings yet
- 2017 Cardiac Disease and Sexuality Implications For 2007 Nursing Clinics of NorDocument11 pages2017 Cardiac Disease and Sexuality Implications For 2007 Nursing Clinics of NorAngie OvandoNo ratings yet
- O U M H: Regional Approaches To Male Health DisparityDocument17 pagesO U M H: Regional Approaches To Male Health DisparityOmar JimenezNo ratings yet
- Writing Task 1 Heart AttackDocument1 pageWriting Task 1 Heart AttackHamzah Insan GemintangNo ratings yet
- Lung CancerDocument10 pagesLung CancerYERALDIN GÓMEZNo ratings yet
- NIH Public AccessDocument16 pagesNIH Public AccessaudiNo ratings yet
- Gender Differences in Disease Manifestation and PresentationDocument5 pagesGender Differences in Disease Manifestation and PresentationGustavo Anzola100% (1)
- Congestive Heart FailureDocument15 pagesCongestive Heart FailureChiraz Mwangi100% (1)
- Stroke RevistedDocument11 pagesStroke Revistedjosephmainam9No ratings yet
- The Michael C Carlos ExperienceDocument2 pagesThe Michael C Carlos Experiencetswag2014No ratings yet
- Business Info Quiz Chapter 3&4Document16 pagesBusiness Info Quiz Chapter 3&4tswag2014No ratings yet
- Everyday Use PaperDocument3 pagesEveryday Use Papertswag2014No ratings yet
- SOA Whitepaper enablingRealWorldSOAthroughtheMicrosoftPlatformDocument22 pagesSOA Whitepaper enablingRealWorldSOAthroughtheMicrosoftPlatformakshatsharma80No ratings yet
- Cis 590 Project Deliverable 6 Final Project Plan 51Document33 pagesCis 590 Project Deliverable 6 Final Project Plan 51tswag2014No ratings yet
- Confucius - The AnalectsDocument3 pagesConfucius - The Analectstswag2014No ratings yet
- Should Sex Ed Start in Middle SchoolDocument4 pagesShould Sex Ed Start in Middle Schooltswag201450% (6)
- ACC 557 Week 4 Chapter 6 E6 1 E6 10 E6 14 P6 3ADocument7 pagesACC 557 Week 4 Chapter 6 E6 1 E6 10 E6 14 P6 3Atswag2014No ratings yet
- Cis 590 Project Deliverable 6 Final Project Plan 51Document33 pagesCis 590 Project Deliverable 6 Final Project Plan 51tswag2014No ratings yet
- ACC 557 Week 5 QuizDocument5 pagesACC 557 Week 5 Quiztswag2014No ratings yet
- Mat540 Quiz 2Document27 pagesMat540 Quiz 2tswag2014No ratings yet
- Mat540 Quiz 2Document27 pagesMat540 Quiz 2tswag2014No ratings yet
- Scientific Programme 18th APCC 090311Document33 pagesScientific Programme 18th APCC 090311drsmiNo ratings yet
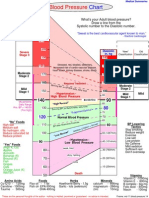
- Blood Pressure ChartDocument1 pageBlood Pressure ChartKAKKAMPI94% (16)
- Ritalin LaDocument20 pagesRitalin Lamichele.siciliano4467No ratings yet
- Diet CounsellingDocument11 pagesDiet CounsellingDrBhawna AroraNo ratings yet
- Discuss What Resources Are Often Necessary For Nonacute Care For Cardiorespiratory IssuesDocument2 pagesDiscuss What Resources Are Often Necessary For Nonacute Care For Cardiorespiratory IssuesBettNo ratings yet
- Fitness Education For ChildrenDocument272 pagesFitness Education For Childrensundar prabhu100% (2)
- Non Communicable DiseaseDocument50 pagesNon Communicable DiseaseLemlem ArgawNo ratings yet
- Initial Data Base For Family Nursing PracticeDocument13 pagesInitial Data Base For Family Nursing PracticeGamer Doge100% (1)
- Paediatric Exercise Science and Medicine, 2 EditionDocument669 pagesPaediatric Exercise Science and Medicine, 2 EditionFlávia AquinoNo ratings yet
- Fitness Assessment ManualDocument266 pagesFitness Assessment ManualVanessa Irene100% (1)
- Asympotmatic Atherosclerosis - Pathophysiology, Detection and Treatment - M. Naghavi (Humana, 2010) WW PDFDocument710 pagesAsympotmatic Atherosclerosis - Pathophysiology, Detection and Treatment - M. Naghavi (Humana, 2010) WW PDFGeorge DanilaNo ratings yet
- Textbook Gizi BDocument20 pagesTextbook Gizi BShirley KawengianNo ratings yet
- Globalization and Its Impact On HealthDocument17 pagesGlobalization and Its Impact On HealthAbdur RahmanNo ratings yet
- Coffee Can Improve Energy Levels and Make You Smarter: 1 2 Caffeine 3Document10 pagesCoffee Can Improve Energy Levels and Make You Smarter: 1 2 Caffeine 3Rengie GaloNo ratings yet
- Cardiac RehabilitationDocument15 pagesCardiac RehabilitationAshraf MullaNo ratings yet
- DermatitisDocument299 pagesDermatitisRudianto AhmadNo ratings yet
- UNIT 3 BookletDocument26 pagesUNIT 3 BookletsglanvillNo ratings yet
- SJ BDJ 2008 850Document13 pagesSJ BDJ 2008 850Mostafa FayadNo ratings yet
- GENES ROLE IN CVD (Genomics)Document4 pagesGENES ROLE IN CVD (Genomics)bashirkinza679No ratings yet
- CONCERTA Extended-Release Tablets PILDocument37 pagesCONCERTA Extended-Release Tablets PILRezaul RazibNo ratings yet
- No Tanggal No. Kartu Nama Pes Sex Jenis Pes Diagnosa: MastayahDocument33 pagesNo Tanggal No. Kartu Nama Pes Sex Jenis Pes Diagnosa: MastayahIc-tika Siee ChuabbieNo ratings yet
- Health7 Q4 Mod4 ProgramsAndPoliciesToPreventNon-communicableDiseases 05102021Document22 pagesHealth7 Q4 Mod4 ProgramsAndPoliciesToPreventNon-communicableDiseases 05102021kiahjessieNo ratings yet
- The Top 16 Health Benefits of Grapes: Health Conditions Discover Plan ConnectDocument26 pagesThe Top 16 Health Benefits of Grapes: Health Conditions Discover Plan Connectkarina chaswinNo ratings yet
- Twohig-Bennet & Jones 2018 - Health Benefits of The Great OutdoorsDocument10 pagesTwohig-Bennet & Jones 2018 - Health Benefits of The Great OutdoorsJD SamanezNo ratings yet
- Katy Bowman - Don't Just Sit There-Propriometrics Press (2015)Document78 pagesKaty Bowman - Don't Just Sit There-Propriometrics Press (2015)Jana Henri100% (2)
- Technological University of The PhilippinesDocument5 pagesTechnological University of The PhilippinesIsha BalangueNo ratings yet
- Cardiovascular Disorders - AuriculotherapyDocument3 pagesCardiovascular Disorders - AuriculotherapyCarissa Nichols100% (2)
- g10 Health Unit PlanDocument7 pagesg10 Health Unit Planapi-263590842No ratings yet
- Herbs Content For BrochureDocument9 pagesHerbs Content For BrochureMulayam Singh YadavNo ratings yet
- Personal Trainers Guide Clients' Health ScreeningsDocument18 pagesPersonal Trainers Guide Clients' Health Screeningsgrande napaNo ratings yet