You might also like
- Sample Medical Guidelines: ACLS-BradycardiaDocument2 pagesSample Medical Guidelines: ACLS-BradycardiaCheewin KhawprapaNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani KayedNo ratings yet
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki HartawanNo ratings yet
- Emergency in Medicine 2012Document202 pagesEmergency in Medicine 2012micheal1960No ratings yet
- Arrhythmia: PalpitationDocument36 pagesArrhythmia: PalpitationHala BahaaNo ratings yet
- Cardiac Arrythmias in The ED Menbeu Edited From AnaDocument106 pagesCardiac Arrythmias in The ED Menbeu Edited From AnaTemesgen Geleta100% (1)
- Supraventricular ArrhythmiasDocument56 pagesSupraventricular ArrhythmiasGading AuroraNo ratings yet
- Management of Cardiac Arrhytmia in Advanced Cardiac Life Support (ACLS)Document34 pagesManagement of Cardiac Arrhytmia in Advanced Cardiac Life Support (ACLS)rhezzaagxxNo ratings yet
- Advanced Cardiac Life Support (Acls) Part Ii: ACP 202 Module 6Document32 pagesAdvanced Cardiac Life Support (Acls) Part Ii: ACP 202 Module 6MoeNo ratings yet
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument64 pagesDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyNo ratings yet
- Advanced Cardiovascular Life Support (Acls)Document45 pagesAdvanced Cardiovascular Life Support (Acls)Erinne DefrianiNo ratings yet
- Basic Arrythmias: Prof. Maximin A. Pomperada, RN, MNDocument70 pagesBasic Arrythmias: Prof. Maximin A. Pomperada, RN, MNRellie CastroNo ratings yet
- Med-Surge Study GuideDocument39 pagesMed-Surge Study Guidefbernis1480_11022046No ratings yet
- 5-Approach To PalpitationsDocument103 pages5-Approach To PalpitationsEverythingNo ratings yet
- Allergy and Immunology: Immunodeficiency 10 Warning Signs of ImmunodeficiencyDocument24 pagesAllergy and Immunology: Immunodeficiency 10 Warning Signs of Immunodeficiencyacque100% (2)
- Arrhythmias Sherry Vickers, RN, MSN, CCRNDocument9 pagesArrhythmias Sherry Vickers, RN, MSN, CCRNSydney DeringNo ratings yet
- Approach To PalpitationsDocument74 pagesApproach To PalpitationsDarawan MirzaNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Advanced Cardiac Life Support (Acls) Part Iii: ACP 202 Module 6Document39 pagesAdvanced Cardiac Life Support (Acls) Part Iii: ACP 202 Module 6MoeNo ratings yet
- Basic Echocardiography, MantapDocument54 pagesBasic Echocardiography, MantapDr Edi Hidayat50% (2)
- CardioDocument9 pagesCardioVirgilio Reyes ManuelNo ratings yet
- Cardiology 7 - Arrhythmias: Lecture OutlineDocument6 pagesCardiology 7 - Arrhythmias: Lecture Outlineمحمد احمد محمدNo ratings yet
- Critical Care NursingDocument159 pagesCritical Care NursingJoy Jarin50% (2)
- Cardiac - Potpourri Rev 2015Document80 pagesCardiac - Potpourri Rev 2015Sanaz NikiNo ratings yet
- Acute Coronary Syndrome EditedDocument38 pagesAcute Coronary Syndrome EditedSurgicalgownNo ratings yet
- ShockDocument75 pagesShockaulianmediansyahNo ratings yet
- Topic: Cardiac Arrest Megacode: MD Khairulamin AS Nursing Lecturer PAPRSB Institute of Health Sciences UBDDocument38 pagesTopic: Cardiac Arrest Megacode: MD Khairulamin AS Nursing Lecturer PAPRSB Institute of Health Sciences UBDulipah100% (2)
- Interesting ECG Sharing: Ms. Yiu Sau-Chi, GigiDocument49 pagesInteresting ECG Sharing: Ms. Yiu Sau-Chi, GigiCarmen FongNo ratings yet
- Intern Survival Guide (UIC)Document51 pagesIntern Survival Guide (UIC)medstick100% (1)
- Supplementary Material 4.3 Cardiac Rhythm Disorders-2Document14 pagesSupplementary Material 4.3 Cardiac Rhythm Disorders-2Andrea Love PalomoNo ratings yet
- Synthesis: History Report SBAR Complete PA Know Your Patho!!! Don't Get Caught W/drawersDocument30 pagesSynthesis: History Report SBAR Complete PA Know Your Patho!!! Don't Get Caught W/drawersmmcgee002No ratings yet
- Advanced Cardiac Life Support (ACLS) : By: Diana Blum MSN Metropolitan Community College Nursing 2150Document16 pagesAdvanced Cardiac Life Support (ACLS) : By: Diana Blum MSN Metropolitan Community College Nursing 2150Vikneswara SoorianarayananNo ratings yet
- Ecg in Emergency: Adi SulistyantoDocument41 pagesEcg in Emergency: Adi Sulistyantomech_pilot2203No ratings yet
- Advance Cardiac SuppDocument32 pagesAdvance Cardiac SuppVijith.V.kumarNo ratings yet
- ACLS Algorithms SlideDocument26 pagesACLS Algorithms SlidehrsoNo ratings yet
- Module 1 Case StudyDocument5 pagesModule 1 Case Studyapi-564432337100% (1)
- Cardiac ArrestDocument14 pagesCardiac ArrestCloudySkyNo ratings yet
- Arrhythmia, Pericardial and Myocardial Diseases (DR Praveen) 2Document44 pagesArrhythmia, Pericardial and Myocardial Diseases (DR Praveen) 2hashini1997nisansalaNo ratings yet
- Cardiovascular Library Small GroupDocument33 pagesCardiovascular Library Small GroupSarah SabtiNo ratings yet
- Arrhythmia 6 YrDocument72 pagesArrhythmia 6 YrPiyush MalikNo ratings yet
- ECG-Arrhythmias: Tiang Soon WeeDocument63 pagesECG-Arrhythmias: Tiang Soon WeeasdasdasdasNo ratings yet
- Palpitations: DR Polamuri Tabitha PG First YrDocument37 pagesPalpitations: DR Polamuri Tabitha PG First YrNinaNo ratings yet
- Electroconvulsive Therapy: An UpdateDocument39 pagesElectroconvulsive Therapy: An UpdateAnonymous 83o62cNo ratings yet
- Holter Monitoring: Dr. Kazi Alam NowazDocument19 pagesHolter Monitoring: Dr. Kazi Alam NowazRadison sierraNo ratings yet
- ACLS Pitfalls Osce For ExternDocument35 pagesACLS Pitfalls Osce For ExternKrittin NaravejsakulNo ratings yet
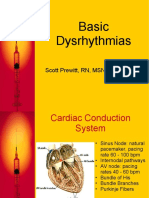
- Basic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCDocument42 pagesBasic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCtuffie85No ratings yet
- Acls Study Guide 2016 For Pulse 2016Document8 pagesAcls Study Guide 2016 For Pulse 2016eng78ineNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- Perfusion, Class 11 ReviewedDocument45 pagesPerfusion, Class 11 ReviewedMelissa GPNo ratings yet
- Dysrhythmias NotesDocument23 pagesDysrhythmias NoteskmimmackNo ratings yet
- ACLS-Pediatric Wide Complex Tachycardia: Sample Medical GuidelinesDocument2 pagesACLS-Pediatric Wide Complex Tachycardia: Sample Medical GuidelinesFebrialitaFatoniNo ratings yet
- Ecg 2Document10 pagesEcg 2AANo ratings yet
- Penyakit Kardiovaskular Yang Sering DijumpaiDocument121 pagesPenyakit Kardiovaskular Yang Sering Dijumpaiandikaagus13No ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- Antiarrhythmic DrugsDocument50 pagesAntiarrhythmic DrugsamirNo ratings yet
- ArrhythmiaDocument31 pagesArrhythmiaAbdallah Essam Al-ZireeniNo ratings yet
- ACLS Algorithms 2011 PDFDocument6 pagesACLS Algorithms 2011 PDFmaya_fitrianaNo ratings yet
- 15 Walters LLSA ArticlesDocument33 pages15 Walters LLSA ArticlesericNo ratings yet
- Chapter 6 IntersubjectivityDocument32 pagesChapter 6 IntersubjectivityWillington Cuaresma67% (3)
- Biological Science Major - Part 1Document9 pagesBiological Science Major - Part 1Willington CuaresmaNo ratings yet
- Manage Chest TubesDocument75 pagesManage Chest TubesWillington CuaresmaNo ratings yet
- Inpt Nursing Adult AssessmentDocument8 pagesInpt Nursing Adult AssessmentWillington Cuaresma100% (1)
- Paternalism Justice Confidentiality VeracityDocument5 pagesPaternalism Justice Confidentiality VeracityWillington CuaresmaNo ratings yet
- Euthanasia - and NonmaleficenceDocument7 pagesEuthanasia - and NonmaleficenceWillington CuaresmaNo ratings yet
- Virtue EthicsDocument2 pagesVirtue EthicsWillington CuaresmaNo ratings yet
- Comprehensive Pharmacy NotesDocument151 pagesComprehensive Pharmacy NotesWillington CuaresmaNo ratings yet
- 1.CD Control Program: RD RDDocument18 pages1.CD Control Program: RD RDKen Mark CatubigNo ratings yet
- Law Rights and JurisprudenceDocument6 pagesLaw Rights and JurisprudenceWillington CuaresmaNo ratings yet
- Glucose Tolerance TestDocument4 pagesGlucose Tolerance TestNikhil KanikaNo ratings yet
- جورنال جاهزDocument4 pagesجورنال جاهزasrd ramiNo ratings yet
- Doenges, Et. Al, (2008) - Nurse's Pocket Guide. 11 Edition. F.A. Davis Company. P. 385Document3 pagesDoenges, Et. Al, (2008) - Nurse's Pocket Guide. 11 Edition. F.A. Davis Company. P. 385Theresa AbrilloNo ratings yet
- Post Polycythemia Vera Myelofibrosis PPV MF A Case Report of A Patient Transplanted After An Adverse Reaction To Covid VaccinationDocument5 pagesPost Polycythemia Vera Myelofibrosis PPV MF A Case Report of A Patient Transplanted After An Adverse Reaction To Covid VaccinationLord 11No ratings yet
- Skin Care and Management of Pressure UlcerDocument24 pagesSkin Care and Management of Pressure UlcerchellczyNo ratings yet
- Prognostic Factors in Tuberculosis Related Mortalities in Hospitalized PatientsDocument7 pagesPrognostic Factors in Tuberculosis Related Mortalities in Hospitalized PatientsAshok PanjwaniNo ratings yet
- 7.1. Anemia 2023Document30 pages7.1. Anemia 2023MichellyTjoaNo ratings yet
- Sabreen Ma K19Document396 pagesSabreen Ma K19Medical ReportNo ratings yet
- Guilford Child & Adolescent Psychology Chapter SamplerDocument97 pagesGuilford Child & Adolescent Psychology Chapter SamplerAdelaKočanBahtoNo ratings yet
- Stroke BrochureDocument2 pagesStroke Brochurenananana123No ratings yet
- Elevator Pitch James Baxter s2896471-3Document1 pageElevator Pitch James Baxter s2896471-3api-335944748No ratings yet
- A Short History of OnchocerciasisDocument12 pagesA Short History of OnchocerciasisAldo Sánchez100% (1)
- Primary Secondary SurveyDocument38 pagesPrimary Secondary SurveySyiema ZainalNo ratings yet
- Spitz Nevi Dan Nodular MelanomaDocument5 pagesSpitz Nevi Dan Nodular MelanomaMeta SakinaNo ratings yet
- Pes Cavus ....Document34 pagesPes Cavus ....Rupika Sodhi100% (2)
- 300+ TOP Digestive System MCQs and Answers PDF Quiz ExamDocument11 pages300+ TOP Digestive System MCQs and Answers PDF Quiz ExamMuhammad AliNo ratings yet
- The Colleges of Medicine of South AfricaDocument4 pagesThe Colleges of Medicine of South AfricaRichard100% (1)
- PUERPERAL SEPSIS CoverDocument9 pagesPUERPERAL SEPSIS CoverKerpersky LogNo ratings yet
- v19 n4Document178 pagesv19 n4Jaa DeeNo ratings yet
- PE - Module 5Document8 pagesPE - Module 5Hanah Grace GomezNo ratings yet
- Weber, J. and Kelley, J. (2018) Health Assessment in Nursing. Sixth EditionDocument18 pagesWeber, J. and Kelley, J. (2018) Health Assessment in Nursing. Sixth EditionClare Collado100% (1)
- ENT DefinationDocument22 pagesENT Definationيدا واحدةNo ratings yet
- Nursing Responsibilities For Oxygen AdministrationDocument3 pagesNursing Responsibilities For Oxygen AdministrationJahseh WolfeNo ratings yet
- Treatment of Chronic Graft-Versus-Host Disease - UpToDateDocument23 pagesTreatment of Chronic Graft-Versus-Host Disease - UpToDatemihaela popescuNo ratings yet
- Applied Biology (PERSONALIZED MEDICINE)Document9 pagesApplied Biology (PERSONALIZED MEDICINE)HAZEL LEELA A P RICHARDNo ratings yet
- Wesleyan: College of Nursing and Allied Medical SciencesDocument2 pagesWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNo ratings yet
- Objective Testing of Pelvic Floor FunctionDocument2 pagesObjective Testing of Pelvic Floor FunctionSteven ElvyNo ratings yet
- Anatomy of The Inguinal RegionDocument24 pagesAnatomy of The Inguinal RegionAhmed ShehadaNo ratings yet
- 00 H&N NotesDocument16 pages00 H&N NotesHythem HashimNo ratings yet
- Anu Omr Long CaseDocument29 pagesAnu Omr Long CaseAnurtha AnuNo ratings yet