You might also like
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Chapter 22 - Management of Patients With Upper Respiratory Tract Disorders (INCOMPLETEon 13)Document16 pagesChapter 22 - Management of Patients With Upper Respiratory Tract Disorders (INCOMPLETEon 13)Mary Singleton100% (1)
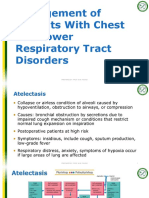
- Chapter 23 - Management of Patients With Chest and Lower Respiratory Tract Disorders (PrepUDONE)Document7 pagesChapter 23 - Management of Patients With Chest and Lower Respiratory Tract Disorders (PrepUDONE)Mary SingletonNo ratings yet
- Post Op Worksheet FinalDocument5 pagesPost Op Worksheet FinalRiza Angela BarazanNo ratings yet
- Concept Map - F and EDocument1 pageConcept Map - F and EAbigail LonoganNo ratings yet
- AtireviewDocument163 pagesAtireviewGlory Mimi0% (1)
- CA1 Module 4 Activities: Lesson 1Document6 pagesCA1 Module 4 Activities: Lesson 1Esmareldah Henry SirueNo ratings yet
- SANITATIONDocument33 pagesSANITATIONLoremma DumlaoNo ratings yet
- Management of Chest and Lower Respiratory DisordersDocument32 pagesManagement of Chest and Lower Respiratory DisordersSam GarciaNo ratings yet
- Oxygen TherapyDocument3 pagesOxygen Therapymarie100% (3)
- NCM 116 Lab Midterm ActivityDocument2 pagesNCM 116 Lab Midterm ActivityEula Dannah Alyssha EboraNo ratings yet
- NCM 10411Document30 pagesNCM 10411jonas2663No ratings yet
- Chapter 39 - Assessment and Management of Patients With Hepatic DisordersDocument6 pagesChapter 39 - Assessment and Management of Patients With Hepatic DisordersMichael BoadoNo ratings yet
- Central Venous Pressure MonitoringDocument2 pagesCentral Venous Pressure MonitoringpauchanmnlNo ratings yet
- Week 10 - Ch. 38 - OxygenationDocument36 pagesWeek 10 - Ch. 38 - OxygenationMary SingletonNo ratings yet
- Case Scenarios on Preoperative, Intraoperative and Postoperative AssessmentsDocument2 pagesCase Scenarios on Preoperative, Intraoperative and Postoperative Assessmentshamisi100% (1)
- M Vanguardia-McnpDocument11 pagesM Vanguardia-Mcnpmark OrpillaNo ratings yet
- FUNDAMENTALSAnswer and RationaleDocument20 pagesFUNDAMENTALSAnswer and RationaleRandyNo ratings yet
- NCM103 - 2016 - Lecture2 - Response To Altered Respiratory FunctionDocument128 pagesNCM103 - 2016 - Lecture2 - Response To Altered Respiratory FunctionrimeoznekNo ratings yet
- Leadership & Management in Nursing NCLEX Practice Quiz (80 Questions)Document38 pagesLeadership & Management in Nursing NCLEX Practice Quiz (80 Questions)Mack MakaNo ratings yet
- Medical Surgical Nursing Review Questions Part 3Document8 pagesMedical Surgical Nursing Review Questions Part 3angelfire23phNo ratings yet
- Are You Kidding MeDocument10 pagesAre You Kidding MeChelsea RoseNo ratings yet
- Jurisprudence QuestionDocument5 pagesJurisprudence QuestionRie Gumiit PimentelNo ratings yet
- Rhea TestDocument3 pagesRhea Testerma090308No ratings yet
- Provide assistancein activities of dailyliving as needed toconserve energy forrespirationDocument6 pagesProvide assistancein activities of dailyliving as needed toconserve energy forrespirationCuttie Anne GalangNo ratings yet
- 60 91 EndocrineDocument34 pages60 91 EndocrineYaj CruzadaNo ratings yet
- Periop QuizesDocument9 pagesPeriop QuizesAnonymous ZQ4gHahzNo ratings yet
- Nurse Prepared with Task and Quality CareDocument22 pagesNurse Prepared with Task and Quality CareLorcan Soi100% (1)
- Pnle 1-Foundation of Professional NSG PracticeDocument19 pagesPnle 1-Foundation of Professional NSG Practiceshiela maeNo ratings yet
- Funda Saved Ms2003Document103 pagesFunda Saved Ms2003June DumdumayaNo ratings yet
- Medical-Surgical Nursing (Gastrointestinal)Document1 pageMedical-Surgical Nursing (Gastrointestinal)アンナドミニクNo ratings yet
- Congestive Heart Failure OutlineDocument4 pagesCongestive Heart Failure OutlineDominique PorterNo ratings yet
- MCN II AntepartumDocument28 pagesMCN II AntepartumJharaNo ratings yet
- Type and Indication of IV Therapy 2Document33 pagesType and Indication of IV Therapy 2Ruth Jazelle MendozaNo ratings yet
- NursingBulletin Notes On PneumothoraxDocument27 pagesNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- Grand Coaching: Medical Surgical NursingDocument22 pagesGrand Coaching: Medical Surgical NursingEsarpy (Nana)No ratings yet
- Emergency Cardiac Medications for ArrhythmiasDocument14 pagesEmergency Cardiac Medications for ArrhythmiasRomzy BasañesNo ratings yet
- 8 Irrigating A ColostomyDocument5 pages8 Irrigating A ColostomyAnn Jalover PerezNo ratings yet
- MS 1ST & 2ND Term ExamDocument114 pagesMS 1ST & 2ND Term ExamKathleen Dela CruzNo ratings yet
- Chapter 16Document10 pagesChapter 16missy23pap50% (2)
- MedSurg 2Document69 pagesMedSurg 2Claire Maurice JuaneroNo ratings yet
- Emergency Nursing Assessment QuestionsDocument10 pagesEmergency Nursing Assessment QuestionsTni JolieNo ratings yet
- Board Questions 2009Document16 pagesBoard Questions 2009Erick EspinoNo ratings yet
- Chapter 18Document11 pagesChapter 18missy23pap100% (1)
- November 2008 PreboardDocument84 pagesNovember 2008 PreboardYaj CruzadaNo ratings yet
- Aging Perspective and Demography Ncm114 Gerontology Aging PerspectivesDocument19 pagesAging Perspective and Demography Ncm114 Gerontology Aging PerspectivesLeslie CruzNo ratings yet
- Psychiatric Nursing Drills for Child Abuse VictimsDocument7 pagesPsychiatric Nursing Drills for Child Abuse Victimsstoto_arenNo ratings yet
- NCM 31112L Midterm Exams: RationalizationDocument202 pagesNCM 31112L Midterm Exams: RationalizationWen SilverNo ratings yet
- De Sagun, Leila Camille, A. NCMB312-RLE BSN3Y1-1B Course Task #1Document1 pageDe Sagun, Leila Camille, A. NCMB312-RLE BSN3Y1-1B Course Task #1Carl SantosNo ratings yet
- Intra-Abdominal Pressure: Causes, Symptoms and TreatmentDocument29 pagesIntra-Abdominal Pressure: Causes, Symptoms and TreatmentRoshin Mae E. TejeroNo ratings yet
- PANCREATITISDocument38 pagesPANCREATITISVEDHIKAVIJAYANNo ratings yet
- CNO-Compendium: Understanding Ethical FrameworksDocument42 pagesCNO-Compendium: Understanding Ethical FrameworksdanushaNo ratings yet
- Test Your Nursing Knowledge: CA1 Module 3 ActivitiesDocument6 pagesTest Your Nursing Knowledge: CA1 Module 3 ActivitiesEsmareldah Henry SirueNo ratings yet
- Pentagon Review - Nursing ManagementDocument5 pagesPentagon Review - Nursing ManagementJay ReanoNo ratings yet
- Recalls 7 CompilationDocument117 pagesRecalls 7 CompilationReka LambinoNo ratings yet
- OXYGENATIONDocument8 pagesOXYGENATIONJo Marchianne Pigar0% (1)
- NP3 ExamDocument14 pagesNP3 ExamArnie Jude CaridoNo ratings yet
- Er 1Document8 pagesEr 1Justin HannahNo ratings yet
- Managing Chest and Lower Respiratory DisordersDocument5 pagesManaging Chest and Lower Respiratory DisordersMary SingletonNo ratings yet
- APA Challenges of Single Parent2Document8 pagesAPA Challenges of Single Parent2Mary SingletonNo ratings yet
- Time Management InstrumentDocument2 pagesTime Management InstrumentMary SingletonNo ratings yet
- Rubric - Safety AssignmentDocument2 pagesRubric - Safety AssignmentMary SingletonNo ratings yet
- Yummy Yummy Gummy in My TummyDocument1 pageYummy Yummy Gummy in My TummyMary SingletonNo ratings yet
- Week03 PeerReviewedEssayDocument4 pagesWeek03 PeerReviewedEssayMary SingletonNo ratings yet
- Chapter 004Document3 pagesChapter 004Mary SingletonNo ratings yet
- Human Development Nursing QuestionsDocument12 pagesHuman Development Nursing QuestionsMary SingletonNo ratings yet
- TelSUMMER 2017 NURS 302 Health Teaching Syllabus - SsDocument16 pagesTelSUMMER 2017 NURS 302 Health Teaching Syllabus - SsMary SingletonNo ratings yet
- Social Movements and Technology Drive ChangeDocument35 pagesSocial Movements and Technology Drive ChangeMary SingletonNo ratings yet
- IMDb Movie Glossary GuideDocument14 pagesIMDb Movie Glossary GuideMary SingletonNo ratings yet
- Math Equation Sheet PDFDocument3 pagesMath Equation Sheet PDFMary SingletonNo ratings yet
- Tooth DecayDocument28 pagesTooth DecayRyan Carlo CondeNo ratings yet
- Benokraitis SOC3 CH 8Document55 pagesBenokraitis SOC3 CH 8Mary SingletonNo ratings yet
- Provide:: Suicide Fighting and Aggression Vehicular AccidentsDocument2 pagesProvide:: Suicide Fighting and Aggression Vehicular AccidentsMary SingletonNo ratings yet
- Syllabus FLM - 307 Fall 2016Document21 pagesSyllabus FLM - 307 Fall 2016Mary SingletonNo ratings yet
- You Can Grow Your BrainDocument1 pageYou Can Grow Your BrainMary SingletonNo ratings yet
- Legal Dimensions of Nursing PracticeDocument25 pagesLegal Dimensions of Nursing PracticeMary SingletonNo ratings yet
- Change APADocument4 pagesChange APAMary SingletonNo ratings yet
- Week 4 - Ch. 12 - DiagnosingDocument16 pagesWeek 4 - Ch. 12 - DiagnosingMary SingletonNo ratings yet
- Chapter 39 - Fluid, Electrolyte, and Acid-Base BalanceDocument41 pagesChapter 39 - Fluid, Electrolyte, and Acid-Base BalanceMary Singleton100% (1)
- Who's paying bills? Consent for financesDocument2 pagesWho's paying bills? Consent for financesMary SingletonNo ratings yet
- PC Shifting Paradigm Kelley and MeierDocument2 pagesPC Shifting Paradigm Kelley and MeierMary SingletonNo ratings yet
- Week 7 - Ch. 20 - CommunicatorDocument23 pagesWeek 7 - Ch. 20 - CommunicatorMary SingletonNo ratings yet
- Week 8 - Ch. 22 - LeaderDocument23 pagesWeek 8 - Ch. 22 - LeaderMary SingletonNo ratings yet
- Week 4 - Ch. 11 - AssessingDocument22 pagesWeek 4 - Ch. 11 - AssessingMary SingletonNo ratings yet
- Week 5 - Ch. 15 - EvaluateDocument17 pagesWeek 5 - Ch. 15 - EvaluateMary SingletonNo ratings yet
- Week 10 - Ch. 38 - OxygenationDocument36 pagesWeek 10 - Ch. 38 - OxygenationMary SingletonNo ratings yet
- Week 7 - Ch. 21 - TeacherDocument25 pagesWeek 7 - Ch. 21 - TeacherMary SingletonNo ratings yet
- Week 11 - Ch. 36 - UrinaryDocument27 pagesWeek 11 - Ch. 36 - UrinaryMary SingletonNo ratings yet
- Advocacy Survey QuestionsDocument2 pagesAdvocacy Survey QuestionsMary SingletonNo ratings yet
- L P 10Document13 pagesL P 10Bình Minh HoàngNo ratings yet
- Snorkeling: A Brief History and Guide to This Underwater AdventureDocument3 pagesSnorkeling: A Brief History and Guide to This Underwater AdventureBernadette PerezNo ratings yet
- Alfa Romeo Giulia Range and Quadrifoglio PricelistDocument15 pagesAlfa Romeo Giulia Range and Quadrifoglio PricelistdanielNo ratings yet
- Philip Larkin: The Art of Poetry 30Document32 pagesPhilip Larkin: The Art of Poetry 30Telmo RodriguesNo ratings yet
- Assignment of A Glass Transition Temperature Using Thermomechanical Analysis: Tension MethodDocument4 pagesAssignment of A Glass Transition Temperature Using Thermomechanical Analysis: Tension MethodEric GozzerNo ratings yet
- Filler SlabDocument4 pagesFiller Slabthusiyanthanp100% (1)
- Chapter 7 - The Political SelfDocument6 pagesChapter 7 - The Political SelfJohn Rey A. TubieronNo ratings yet
- Symasym BBDocument37 pagesSymasym BBChandraRizkyNo ratings yet
- Project Planning and Management Unit 1Document13 pagesProject Planning and Management Unit 1Savant100% (1)
- GSMA Moile Money Philippines Case Study V X21 21Document23 pagesGSMA Moile Money Philippines Case Study V X21 21davidcloud99No ratings yet
- Ifatsea Atsep Brochure 2019 PDFDocument4 pagesIfatsea Atsep Brochure 2019 PDFCondor GuatonNo ratings yet
- WBC Study Reveals God's NatureDocument11 pagesWBC Study Reveals God's NatureSherwin Castillo DelgadoNo ratings yet
- Professional Builder - Agosto 2014Document32 pagesProfessional Builder - Agosto 2014ValNo ratings yet
- Chapter 4. Quality Service and Standards TrainingDocument40 pagesChapter 4. Quality Service and Standards TrainingJia Mae Sapico ApantiNo ratings yet
- Elements of Ayurveda Daily Routine GuideDocument1 pageElements of Ayurveda Daily Routine GuideShivani GargNo ratings yet
- Primary 2 (Grade 2) - GEP Practice: Contest Problems With Full SolutionsDocument24 pagesPrimary 2 (Grade 2) - GEP Practice: Contest Problems With Full Solutionswenxinyu1002100% (1)
- War, Rivalry An State Building in Latin AmericaDocument16 pagesWar, Rivalry An State Building in Latin AmericaPablo Andrés Garrido GonzálezNo ratings yet
- Activities/Assessments 2:: Determine The Type of Sampling. (Ex. Simple Random Sampling, Purposive Sampling)Document2 pagesActivities/Assessments 2:: Determine The Type of Sampling. (Ex. Simple Random Sampling, Purposive Sampling)John Philip Echevarria0% (2)
- Robotic End Effectors - Payload Vs Grip ForceDocument8 pagesRobotic End Effectors - Payload Vs Grip ForcesamirNo ratings yet
- Horizontal Vertical MarketDocument4 pagesHorizontal Vertical MarketVikasNo ratings yet
- Bahasa InggrisDocument8 pagesBahasa InggrisArintaChairaniBanurea33% (3)
- RA 5921 and RA 10918Document32 pagesRA 5921 and RA 10918Hani Loveres100% (1)
- Amna Hameed: ObjectiveDocument2 pagesAmna Hameed: ObjectiveSabrina GandapurNo ratings yet
- Journal 082013Document100 pagesJournal 082013Javier Farias Vera100% (1)
- E.bs 3rd-Unit 22Document46 pagesE.bs 3rd-Unit 22DUONG LE THI THUYNo ratings yet
- User Manual LCD Signature Pad Signotec SigmaDocument15 pagesUser Manual LCD Signature Pad Signotec SigmaGael OmgbaNo ratings yet
- Barry Wylant: Design Thinking and The Experience of InnovationDocument13 pagesBarry Wylant: Design Thinking and The Experience of InnovationVanesa JuarezNo ratings yet
- Clustering Social Network GraphsDocument12 pagesClustering Social Network GraphsRáhùl SréédhãrNo ratings yet
- Digitrip 520Document40 pagesDigitrip 520HACNo ratings yet
- Product Manual 82434 (Revision C) : Generator Loading ControlDocument26 pagesProduct Manual 82434 (Revision C) : Generator Loading ControlAUGUSTA WIBI ARDIKTANo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)