You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Spreads Through The Major ArcanaDocument29 pagesSpreads Through The Major Arcanaaamir100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Cheatsheet Bias CheatsheetDocument4 pagesCheatsheet Bias CheatsheetRaz WidrichNo ratings yet
- Goals of Local HistoryDocument11 pagesGoals of Local HistoryAngelo Dizon Cabreros100% (1)
- En9Lc-Ivh-2.15: Evaluating BooksDocument3 pagesEn9Lc-Ivh-2.15: Evaluating BooksNIMFA SEPARANo ratings yet
- Methodology in Business Ethics Research A Review PDFDocument15 pagesMethodology in Business Ethics Research A Review PDFMercedes Baño HifóngNo ratings yet
- New Year 2023Document52 pagesNew Year 2023balayogivNo ratings yet
- Safety Information Notice: Subject: General Flight Safety of Helicopters - Issue of EHEST LeafletDocument21 pagesSafety Information Notice: Subject: General Flight Safety of Helicopters - Issue of EHEST LeafletFidel ArellanoNo ratings yet
- American Media Bias FinalDocument8 pagesAmerican Media Bias Finalapi-286287370No ratings yet
- Module 6 Media and Information LanguagesDocument10 pagesModule 6 Media and Information LanguagesLeo Nino DulceNo ratings yet
- JPE Reports For General Assembly 2016Document192 pagesJPE Reports For General Assembly 2016Fauquier NowNo ratings yet
- Reading in Philippine History 1Document19 pagesReading in Philippine History 1Lea Amor Martinez EshedoNo ratings yet
- Religious Syncretism in Spanish Latin America Survival Power ADocument27 pagesReligious Syncretism in Spanish Latin America Survival Power AIan EggheadNo ratings yet
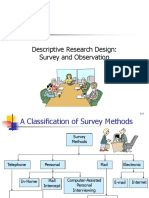
- Descriptive Methods - SurveyDocument23 pagesDescriptive Methods - SurveyPriya GunaNo ratings yet
- Creating Reality - How TV News Distorts EventsDocument4 pagesCreating Reality - How TV News Distorts Eventskiran-z-1972No ratings yet
- Moral ReasoningDocument21 pagesMoral ReasoningDr-Shefali GargNo ratings yet
- Perceptia - Barbara A. Budjac Corvette - Conflict Management - A Practical Guide To Developing Negotiation Strategies-Pearson (2006) - 8Document15 pagesPerceptia - Barbara A. Budjac Corvette - Conflict Management - A Practical Guide To Developing Negotiation Strategies-Pearson (2006) - 8Mădă RădoiNo ratings yet
- Info Sheet IA Guide FIrst Exams 2017 2 3Document15 pagesInfo Sheet IA Guide FIrst Exams 2017 2 3KatrinaNo ratings yet
- Carter Allen - Analysis EssayDocument4 pagesCarter Allen - Analysis EssayCarter AllenNo ratings yet
- Evaluating Childrens Literature Checklist Excel SpreadsheetDocument5 pagesEvaluating Childrens Literature Checklist Excel SpreadsheetTristaNo ratings yet
- Accounting Standard Setting and Its Economic ConsequencesDocument18 pagesAccounting Standard Setting and Its Economic ConsequencesFabian QuincheNo ratings yet
- Teaching-Guide-Catchup-English 8Document2 pagesTeaching-Guide-Catchup-English 8Mayette Danias MondaloNo ratings yet
- Q2 English 6 Module 2 - EditedDocument21 pagesQ2 English 6 Module 2 - EditedMyra Domondon100% (1)
- The Ethical Implications of Artificial IntelligenceDocument2 pagesThe Ethical Implications of Artificial IntelligenceASUS VivoNo ratings yet
- Study Unit 1: Introduction To Psychological AssessmentDocument46 pagesStudy Unit 1: Introduction To Psychological AssessmentThembelani Mlotya X-stainNo ratings yet
- Jensen Shoes common judging shortcuts case studyDocument8 pagesJensen Shoes common judging shortcuts case studyParikshitMishraNo ratings yet
- 6 STDM Course Outline PGP Term 4 2019-20 PDFDocument10 pages6 STDM Course Outline PGP Term 4 2019-20 PDFAkshayNo ratings yet
- Media BiasDocument25 pagesMedia BiasgefrancaNo ratings yet
- Miskeyed Items: Table 8.6 P-Values For A Miskeyed Test ItemDocument30 pagesMiskeyed Items: Table 8.6 P-Values For A Miskeyed Test ItemSukaina AdibiNo ratings yet
- MODULE GRADE 9 Olga TamayoDocument3 pagesMODULE GRADE 9 Olga TamayoGerome Bautista VInluanNo ratings yet
- Social Psychology: Nimrah Ahmed 13/ OCTOBER/ 2016,17 OCTOBER 2016, 18 OCTOBER 2016 & 19 OCTOBER 2016Document41 pagesSocial Psychology: Nimrah Ahmed 13/ OCTOBER/ 2016,17 OCTOBER 2016, 18 OCTOBER 2016 & 19 OCTOBER 2016Alishbah Khan NiaziiNo ratings yet