You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- SAMPLE Information On RapeDocument2 pagesSAMPLE Information On RapeMay May100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Sample Strong Eras Lor 5-05Document1 pageSample Strong Eras Lor 5-05Raiyan KhanNo ratings yet
- Roadmap To Prayer Lesson 16Document18 pagesRoadmap To Prayer Lesson 16Krisztian KelemenNo ratings yet
- Development of Financial Strategy: Chapter Learning ObjectivesDocument6 pagesDevelopment of Financial Strategy: Chapter Learning ObjectivesDINEO PRUDENCE NONG100% (1)
- 21 CFR Part 11 Complete Guide To International Computer Validation Compliance For Pharmaceutical IndustryDocument287 pages21 CFR Part 11 Complete Guide To International Computer Validation Compliance For Pharmaceutical IndustryFabio Green100% (1)
- Open Data Driving Growth Ingenuity and InnovationDocument36 pagesOpen Data Driving Growth Ingenuity and InnovationAnonymous EBlYNQbiMyNo ratings yet
- General Math Second Quarter Exam ReviewDocument5 pagesGeneral Math Second Quarter Exam ReviewAgnes Ramo100% (1)
- Newborn Antibiotic Guide or Early and Late Onset Sepsis During Birth Episode of Care Revised June 2018Document14 pagesNewborn Antibiotic Guide or Early and Late Onset Sepsis During Birth Episode of Care Revised June 2018Raiyan KhanNo ratings yet
- Miracle Baby: Managing Extremely Preterm Birth in Rural UgandaDocument4 pagesMiracle Baby: Managing Extremely Preterm Birth in Rural UgandaRaiyan KhanNo ratings yet
- Denosumab in MyelomaDocument5 pagesDenosumab in MyelomaRaiyan KhanNo ratings yet
- Prepare For Blood Donation Flyer A4Document1 pagePrepare For Blood Donation Flyer A4Raiyan KhanNo ratings yet
- Clin Infect Dis. 2002 Thomas 46 52Document7 pagesClin Infect Dis. 2002 Thomas 46 52Raiyan KhanNo ratings yet
- Health Pra CRN at LawDocument313 pagesHealth Pra CRN at LawRaiyan KhanNo ratings yet
- LicenseDocument3 pagesLicenseSourav SharmaNo ratings yet
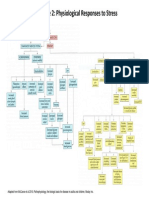
- Figure 2: Physiological Responses To StressDocument1 pageFigure 2: Physiological Responses To StressRaiyan KhanNo ratings yet
- Axis Priority SalaryDocument5 pagesAxis Priority SalarymanojNo ratings yet
- Indies Top Marks For Murder Window Display T&CsDocument1 pageIndies Top Marks For Murder Window Display T&CsSonia RazviNo ratings yet
- Fondazione Prada - January 2019Document6 pagesFondazione Prada - January 2019ArtdataNo ratings yet
- PW Show Daily at Frankfurt Day 1Document68 pagesPW Show Daily at Frankfurt Day 1Publishers WeeklyNo ratings yet
- Akhtar Non IT RecruiterDocument3 pagesAkhtar Non IT RecruiterMohiddinNo ratings yet
- MR - Roleplay RulebookDocument12 pagesMR - Roleplay RulebookMr RoleplayNo ratings yet
- Joseph Stalin: Revisionist BiographyDocument21 pagesJoseph Stalin: Revisionist BiographyStefanoCzarnyNo ratings yet
- Sekolah Menengah Kebangsaan Sultan Abu Bakar, Jalan Beserah, 25300 Kuantan, PahangDocument18 pagesSekolah Menengah Kebangsaan Sultan Abu Bakar, Jalan Beserah, 25300 Kuantan, PahangChandrika RamodaranNo ratings yet
- Customer Accounting and Customer Profitability Analysis For The Order Handling Industry-A Managerial Accounting ApproachDocument13 pagesCustomer Accounting and Customer Profitability Analysis For The Order Handling Industry-A Managerial Accounting ApproachThai HanhNo ratings yet
- Canada Immigration Forms: 5578EDocument7 pagesCanada Immigration Forms: 5578EOleksiy KovyrinNo ratings yet
- Kythera S-1 Ex. 99.1Document471 pagesKythera S-1 Ex. 99.1darwinbondgrahamNo ratings yet
- Clearlake City Council PacketDocument57 pagesClearlake City Council PacketLakeCoNewsNo ratings yet
- WP (C) 267/2012 Etc.: Signature Not VerifiedDocument7 pagesWP (C) 267/2012 Etc.: Signature Not VerifiedAnamika VatsaNo ratings yet
- Culturally Appropriate Communication in Malaysia Budi Bahasa As Warranty Component in Malaysian DiscourseDocument15 pagesCulturally Appropriate Communication in Malaysia Budi Bahasa As Warranty Component in Malaysian DiscourseNur FarihaNo ratings yet
- Benyam Private International LawDocument250 pagesBenyam Private International Lawmuleta100% (2)
- Lost Spring exposes lives of povertyDocument5 pagesLost Spring exposes lives of povertyvandana61No ratings yet
- Airtel A OligopolyDocument43 pagesAirtel A OligopolyMRINAL KAUL100% (1)
- Sharmaji by Anjana AppachanaDocument2 pagesSharmaji by Anjana Appachanasj3No ratings yet
- MCQ Human RightsDocument30 pagesMCQ Human RightsSameer PrasadNo ratings yet
- Artisan Professionnel Program Finds MUA InfluencersDocument7 pagesArtisan Professionnel Program Finds MUA InfluencersWilliam SuriadyNo ratings yet
- Chap 1 ScriptDocument9 pagesChap 1 ScriptDeliza PosadasNo ratings yet
- Literature ReviewDocument6 pagesLiterature Reviewapi-549249112No ratings yet
- Resume for College Professor PositionDocument3 pagesResume for College Professor PositionYours PharmacyNo ratings yet
- Protected Monument ListDocument65 pagesProtected Monument ListJose PerezNo ratings yet