You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Force-Velocity Curve: The Article Explains What The Force-Velocity Curve Is and How To Shift ItDocument8 pagesForce-Velocity Curve: The Article Explains What The Force-Velocity Curve Is and How To Shift Itmehrdad_44No ratings yet
- Which Is The Better Pec BuilderDocument3 pagesWhich Is The Better Pec Buildermehrdad_44No ratings yet
- Set and Rep Schemes in Strength TrainingDocument13 pagesSet and Rep Schemes in Strength Trainingmehrdad_44100% (2)
- The Metabolic Adaptation Manual: Problems, Solutions, and Life After Weight LossDocument88 pagesThe Metabolic Adaptation Manual: Problems, Solutions, and Life After Weight Lossmehrdad_44No ratings yet
- Which Is The Better Pec BuilderDocument3 pagesWhich Is The Better Pec Buildermehrdad_44No ratings yet
- Sex Differences in Lipolysis-Regulating Mechanisms in Overweight Subjects: Effect of Exercise IntensityDocument11 pagesSex Differences in Lipolysis-Regulating Mechanisms in Overweight Subjects: Effect of Exercise Intensitymehrdad_44No ratings yet
- 3 Reasons Your Calves ArenDocument5 pages3 Reasons Your Calves Arenmehrdad_44No ratings yet
- 8 Injections That Heal Injuries - T NationDocument5 pages8 Injections That Heal Injuries - T Nationmehrdad_44No ratings yet
- Band TrainingDocument6 pagesBand Trainingmehrdad_44No ratings yet
- WatermealonDocument5 pagesWatermealonmehrdad_44No ratings yet
- How Fast Should I Run?: Making Use of Your Test DataDocument2 pagesHow Fast Should I Run?: Making Use of Your Test Datamehrdad_44No ratings yet
- Anabolic Steroid Cycles: An Experts Guide To Optimum Use Testosterone: Sprint or Marathon?Document5 pagesAnabolic Steroid Cycles: An Experts Guide To Optimum Use Testosterone: Sprint or Marathon?mehrdad_4450% (2)
- The Natural Muscular Potential of WomenDocument5 pagesThe Natural Muscular Potential of Womenmehrdad_44No ratings yet
- Barbell Squats vs. Smith Machine Squats: Facts of The CaseDocument2 pagesBarbell Squats vs. Smith Machine Squats: Facts of The Casemehrdad_44No ratings yet
- Training Plan Tips From GambettaDocument2 pagesTraining Plan Tips From Gambettamehrdad_44No ratings yet
- How Do Advanced Techniques Affect HypertrophyDocument12 pagesHow Do Advanced Techniques Affect Hypertrophymehrdad_44No ratings yet
- Hip Variation and Customizing Squat StanceDocument10 pagesHip Variation and Customizing Squat Stancemehrdad_44No ratings yet
- How Do Advanced Techniques Affect HypertrophyDocument12 pagesHow Do Advanced Techniques Affect Hypertrophymehrdad_44No ratings yet
- How Could Periodization Help Enhance MuscleDocument9 pagesHow Could Periodization Help Enhance Musclemehrdad_44No ratings yet
- Do You Have the Genetic Potential for BodybuildingDocument6 pagesDo You Have the Genetic Potential for Bodybuildingmehrdad_44No ratings yet
- PercentDocument2 pagesPercentmehrdad_44No ratings yet
- 9 Reasons Why Women Should Not Train Like MenDocument8 pages9 Reasons Why Women Should Not Train Like Menmehrdad_44No ratings yet
- Coaching Instructions and Cues For Enhancing Sprint PerformanceDocument19 pagesCoaching Instructions and Cues For Enhancing Sprint Performancemehrdad_44No ratings yet
- Tip: 25 Ways To Smash Strength PlateausDocument3 pagesTip: 25 Ways To Smash Strength Plateausmehrdad_44100% (1)
- Stretching For RecoveryDocument5 pagesStretching For Recoverymehrdad_44No ratings yet
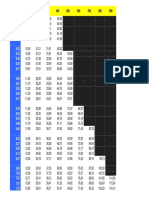
- Distance / V (M/S) 100 200 300 400 500 600 700 800 900Document2 pagesDistance / V (M/S) 100 200 300 400 500 600 700 800 900mehrdad_44No ratings yet
- Elbow Action in SprintingDocument3 pagesElbow Action in Sprintingmehrdad_44No ratings yet
- STRETCH Shortning CycleDocument6 pagesSTRETCH Shortning Cyclemehrdad_44No ratings yet
- Central Concepts Related To PeriodizationDocument6 pagesCentral Concepts Related To Periodizationmehrdad_44No ratings yet
- Microcycle Planning - Blank CECS Level IIIDocument1 pageMicrocycle Planning - Blank CECS Level IIImehrdad_44100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Enthesopathies Knowledge Update - Dreisilker, Ulrich, Dr. MedDocument164 pagesEnthesopathies Knowledge Update - Dreisilker, Ulrich, Dr. MedMarco100% (1)
- WYFL Physical FormDocument2 pagesWYFL Physical FormAshley Nabors TalbotNo ratings yet
- Wound Types and Treatment GuideDocument4 pagesWound Types and Treatment GuideNikki Ann Kanapi FernandezNo ratings yet
- p1k Pde2577tcuk 052009 PDFDocument20 pagesp1k Pde2577tcuk 052009 PDFwalid8311No ratings yet
- Sat Essential Grammar.38-40Document3 pagesSat Essential Grammar.38-40Tijana CurcicNo ratings yet
- TMJDocument40 pagesTMJARIF PUJI LAKSONONo ratings yet
- The Science of ErgonomicsDocument43 pagesThe Science of Ergonomicspoonam_ranee3934No ratings yet
- 1101 1200Document100 pages1101 1200Rj DeciertoNo ratings yet
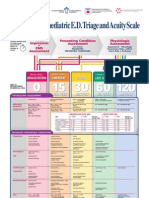
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)
- General principles of first aid aboard shipDocument10 pagesGeneral principles of first aid aboard shipCk DhiyanNo ratings yet
- Dim MakDocument16 pagesDim MakZain ShiraziNo ratings yet
- Oedema Assessment - PhysiopediaDocument12 pagesOedema Assessment - PhysiopediaRafan AddisNo ratings yet
- One Voice, One Heart Prayerfully Ad Lib IntroDocument2 pagesOne Voice, One Heart Prayerfully Ad Lib IntromarkddublinNo ratings yet
- VIPower: VIPer22A Dual Output Reference Board 90 To 264 VAC Input, 10W OutputDocument20 pagesVIPower: VIPer22A Dual Output Reference Board 90 To 264 VAC Input, 10W OutputLullaby summerNo ratings yet
- Surface Anatomy: The Language of AnatomyDocument5 pagesSurface Anatomy: The Language of AnatomyHitagi CrabNo ratings yet
- Management Menyscal PathologyDocument201 pagesManagement Menyscal PathologyMaricruzhdezaNo ratings yet
- GMB Bodyweight CircuitDocument16 pagesGMB Bodyweight Circuitmikevlah100% (1)
- Week 3 Teaching PlanDocument3 pagesWeek 3 Teaching Planapi-339668544No ratings yet
- Spasticity After Stroke 1Document1 pageSpasticity After Stroke 1api-362395776100% (1)
- Saphenous Nerve EntrapmentDocument2 pagesSaphenous Nerve Entrapmentemilio9fernandez9gatNo ratings yet
- Belt Failure AnalysisDocument8 pagesBelt Failure AnalysisDavid ChandlerNo ratings yet
- Back Injuries in ConstructionDocument3 pagesBack Injuries in ConstructionNurNo ratings yet
- Acl Rehab ProtocolDocument37 pagesAcl Rehab ProtocolkhaldoonNo ratings yet
- D - Incident Reporting-RecordingDocument9 pagesD - Incident Reporting-RecordingRaymondGomezBlancoNo ratings yet
- CARETEK Manual Book of Electic Bed User ManualDocument30 pagesCARETEK Manual Book of Electic Bed User ManualaffasdepasterNo ratings yet
- Scapular Dyskinesis: From Basic Science To Ultimate TreatmentDocument17 pagesScapular Dyskinesis: From Basic Science To Ultimate TreatmentAlonso FernandezNo ratings yet
- DAKE Press Model 75 H - 907003Document6 pagesDAKE Press Model 75 H - 907003mark_dayNo ratings yet
- Orbitotomi MedscapeDocument9 pagesOrbitotomi MedscapeBonita AsyigahNo ratings yet
- Final Flight (OCR)Document34 pagesFinal Flight (OCR)Andrés ArceNo ratings yet
- Anatomy & Physiology TissuesDocument13 pagesAnatomy & Physiology TissuesNicole Ken AgdanaNo ratings yet