You might also like
- Practice Essentials: Neonatal HypoglycemiaDocument15 pagesPractice Essentials: Neonatal HypoglycemianadiancupNo ratings yet
- Chapter 22.1 Urea Cycle DefectsDocument3 pagesChapter 22.1 Urea Cycle Defectspriyanshu mathurNo ratings yet
- Maple Syrup Urine Disease (MSUD)Document28 pagesMaple Syrup Urine Disease (MSUD)Dr. Mohammed Al Ja’fari, MDNo ratings yet
- Wikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)Document4 pagesWikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)jcasanovas1995No ratings yet
- Hyperemesis GravidarumDocument21 pagesHyperemesis GravidarumSavita HanamsagarNo ratings yet
- Assignment On TPNDocument14 pagesAssignment On TPNBhawna Joshi100% (8)
- Neonatal HypoglycaemiaDocument29 pagesNeonatal HypoglycaemiarhylesmartNo ratings yet
- Ventilator Basics in The Adult ICUDocument6 pagesVentilator Basics in The Adult ICUnicole289400No ratings yet
- Oxandrolone TabletsDocument5 pagesOxandrolone Tabletsfaqed ilzakiraNo ratings yet
- Pediatric PoisoningDocument47 pagesPediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Total Parenteral Nutrition in NeonatesDocument5 pagesTotal Parenteral Nutrition in NeonatesRisma WatiNo ratings yet
- Fulminant Hepatic FailureDocument8 pagesFulminant Hepatic Failuremiz uNo ratings yet
- Medical ManagementDocument5 pagesMedical ManagementJas Castro JoveroNo ratings yet
- Inborn Error of Metabolism and Introduction To Cancer GeneticsDocument9 pagesInborn Error of Metabolism and Introduction To Cancer GeneticsviancaNo ratings yet
- Metabolic and Inherited DisordersDocument4 pagesMetabolic and Inherited DisordersliggiedyNo ratings yet
- Nucleotide and CHO Metabolism ActivityDocument3 pagesNucleotide and CHO Metabolism ActivityJanson SarmientoNo ratings yet
- C C C CDocument51 pagesC C C CpixiemedicNo ratings yet
- Update On Childhood Diabetes MellitusDocument51 pagesUpdate On Childhood Diabetes MellitusJulie Carnetion DNo ratings yet
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Document4 pagesInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauNo ratings yet
- SCADDDocument4 pagesSCADDRajiv Kabad0% (1)
- Diabetes Mellitus Prepared By: LORI R. LARA, R.NDocument14 pagesDiabetes Mellitus Prepared By: LORI R. LARA, R.NNovie Carla0% (1)
- All Types of InsulinDocument18 pagesAll Types of Insulinali mohammedNo ratings yet
- Chapter 22.2 Organic AcidemiasDocument3 pagesChapter 22.2 Organic Acidemiaspriyanshu mathurNo ratings yet
- Diabetic Ketoacidosis Case StudyDocument6 pagesDiabetic Ketoacidosis Case StudyJohn AlcantaraNo ratings yet
- Diabetic Ketoacidosis Case StudyDocument6 pagesDiabetic Ketoacidosis Case StudyHomework Ping100% (2)
- Acute Liver Failure in ChildrenDocument34 pagesAcute Liver Failure in ChildrenEpahNo ratings yet
- Name of The Medicinal ProductDocument7 pagesName of The Medicinal Productddandan_2No ratings yet
- Refeeding Syndrome GuidelineDocument5 pagesRefeeding Syndrome GuidelinePejman AhmadiNo ratings yet
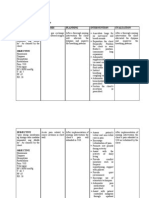
- Nursing Care Plan: DiagnosisDocument11 pagesNursing Care Plan: DiagnosisCharmaine100% (1)
- 1 s2.0 S0749072014000310 MainDocument7 pages1 s2.0 S0749072014000310 MainGustavo Prez CuenkNo ratings yet
- 100Document14 pages100Mohammed BISHRNo ratings yet
- Iem India Perspective N B Kumta MaharashtraDocument8 pagesIem India Perspective N B Kumta Maharashtraavijitcu2007No ratings yet
- NCP Diabetes Mellitus Prepregnancy GestationalDocument12 pagesNCP Diabetes Mellitus Prepregnancy GestationalRichson BacayNo ratings yet
- Presented by DR Ashish Sharma Guided by DR Meena PatelDocument74 pagesPresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccNo ratings yet
- Inborn Errors of Metabolism: Intensive Care Nursery House Staff ManualDocument5 pagesInborn Errors of Metabolism: Intensive Care Nursery House Staff ManualwarishNo ratings yet
- MS3 Review NotesDocument11 pagesMS3 Review NotesPaul Anthony LoricaNo ratings yet
- Maple Syrup Urine DiseaseDocument14 pagesMaple Syrup Urine DiseasefantasticoolNo ratings yet
- Inborn Error of MetabolismDocument55 pagesInborn Error of MetabolismRahil singh chauhanNo ratings yet
- Carbohydrates Metabolism and Diabetes MellitusDocument63 pagesCarbohydrates Metabolism and Diabetes Mellitusapi-19641337No ratings yet
- Report DISORDERS OF MALABSORPTIONDocument8 pagesReport DISORDERS OF MALABSORPTIONKathleen Anzhelika B. NemenzoNo ratings yet
- Diabetic Ketoacidosis Case StudyDocument5 pagesDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- 6 - Inborn Errors of Metabolism - Spring 23Document42 pages6 - Inborn Errors of Metabolism - Spring 23Abdo HaiderNo ratings yet
- Neonatal SeizuresDocument6 pagesNeonatal SeizuresClaraAmeliaNo ratings yet
- Drug StudyDocument5 pagesDrug StudyAl-nazer Azer AlNo ratings yet
- Metabolic Alkalosis: Features of Crohn'S DiseaseDocument15 pagesMetabolic Alkalosis: Features of Crohn'S DiseaseRajiv Kabad100% (1)
- Hypocalcemia Is A Laboratory and Clinical Abnormality That Is Observed With Relative FrequencyDocument3 pagesHypocalcemia Is A Laboratory and Clinical Abnormality That Is Observed With Relative FrequencySuzetteBragaSamuelaNo ratings yet
- Persistent Diarrhea With Severe Malnutrition Type MarasmusDocument47 pagesPersistent Diarrhea With Severe Malnutrition Type MarasmusAkash KhannaNo ratings yet
- Dark Mode Project Kanban Board Brainstorm PresentationDocument11 pagesDark Mode Project Kanban Board Brainstorm Presentationnadzwa velascoNo ratings yet
- New Hypoglycmemia 1Document61 pagesNew Hypoglycmemia 1Suravi DuttaNo ratings yet
- EmesisDocument25 pagesEmesisShista PriyadarshiniNo ratings yet
- Acute Kidney Injury (Aki) : MBCHB ViDocument25 pagesAcute Kidney Injury (Aki) : MBCHB ViENOCK BENDERENo ratings yet
- All About Anorexia in The Elderly: Czeresna H. SoejonoDocument5 pagesAll About Anorexia in The Elderly: Czeresna H. SoejonoJalu PanjongkoNo ratings yet
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- A Seminar On Hypoglycemia: Debremarkos University School of MedicineDocument59 pagesA Seminar On Hypoglycemia: Debremarkos University School of MedicinewoldemariamNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- The #1 Danger Of Prolonged Fasting You Have To Know About - Based On The Teachings Of Dr. Eric Berg: The Most Important Risk To UnderstandFrom EverandThe #1 Danger Of Prolonged Fasting You Have To Know About - Based On The Teachings Of Dr. Eric Berg: The Most Important Risk To UnderstandNo ratings yet
- Solutions to Diabetes and Hypoglycemia (Translated): How to prevent and get rid of it in a natural way, without resorting to medicines but adopting a correct way of lifeFrom EverandSolutions to Diabetes and Hypoglycemia (Translated): How to prevent and get rid of it in a natural way, without resorting to medicines but adopting a correct way of lifeNo ratings yet
- The Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorDocument11 pagesThe Sadomasochism Checklist: A Tool For The Assessment of Sadomasochistic BehaviorMichael Tavera OsorioNo ratings yet
- P ValueDocument6 pagesP ValuemkmznsNo ratings yet
- Compact Unit Faecal Sludge - EnglishDocument2 pagesCompact Unit Faecal Sludge - EnglishHussam MostafaNo ratings yet
- Healthy Diet Plans (Anemia)Document21 pagesHealthy Diet Plans (Anemia)Rohan GulavaniNo ratings yet
- Malignant MelanomaDocument31 pagesMalignant MelanomakityamuwesiNo ratings yet
- The Effects of Functional Training, Bicycle Exercise and Exergaming On Walking Capacity of Elderly With Parkinson's Disease A PDocument28 pagesThe Effects of Functional Training, Bicycle Exercise and Exergaming On Walking Capacity of Elderly With Parkinson's Disease A PabcsouzaNo ratings yet
- Surgeon's ReportDocument2 pagesSurgeon's ReportjalenNo ratings yet
- Non Hodgkin Lymphoma in ChildrenDocument4 pagesNon Hodgkin Lymphoma in ChildrenMilzan MurtadhaNo ratings yet
- Introduction of Abbott LaboratoriesDocument9 pagesIntroduction of Abbott LaboratoriesAhsan AliNo ratings yet
- RTA Type 1 TreatmentDocument4 pagesRTA Type 1 TreatmentJane RamosNo ratings yet
- NURSING CARE PLAN Lung Cancer..jonardDocument2 pagesNURSING CARE PLAN Lung Cancer..jonardJ.C. Kate Cruz67% (3)
- Applejuice As DegreaserDocument26 pagesApplejuice As DegreaserKaryle Anne Surban TabianNo ratings yet
- Usepa 2014Document16 pagesUsepa 2014walidNo ratings yet
- "My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheDocument4 pages"My Neck Feels Stiff and There's Pain Coming From It. Every Time I Move It, It Only Gets Worse." As Stated by TheCassey CuregNo ratings yet
- COPD Lecture Slides For BlackBoardDocument52 pagesCOPD Lecture Slides For BlackBoardClayton JensenNo ratings yet
- CBT βιβλίαDocument24 pagesCBT βιβλίαEliza KottikaNo ratings yet
- PFOADocument4 pagesPFOAVaishali RaneNo ratings yet
- Resume UpdatedDocument2 pagesResume Updatedapi-253794925No ratings yet
- PathophysiologyDocument13 pagesPathophysiologyJan Phi LipNo ratings yet
- Surgical DressingDocument2 pagesSurgical Dressinggao1989No ratings yet
- 1954 01 01 Mosquito Control ReportDocument2 pages1954 01 01 Mosquito Control Reportkbreenbo1No ratings yet
- Non-Surgical Periodontal Therapy Part 1 PDFDocument106 pagesNon-Surgical Periodontal Therapy Part 1 PDFnsr_sweetyNo ratings yet
- Asthma IhpDocument2 pagesAsthma Ihpapi-454842648No ratings yet
- 8-Veria Technique of Cochlear Implantation Our ExperienceDocument4 pages8-Veria Technique of Cochlear Implantation Our ExperienceAnonymous ST1Ot2GAHxNo ratings yet
- DR - Abeidi's Review FinalDocument157 pagesDR - Abeidi's Review FinalSandra AbboudNo ratings yet
- SOP - Statement of PurposeDocument3 pagesSOP - Statement of PurposeAli Zain50% (2)
- Self Sustainable Integrated Township: A Resource-Based Planning To Improve The Quality of Urban LifeDocument24 pagesSelf Sustainable Integrated Township: A Resource-Based Planning To Improve The Quality of Urban Lifewahid kallidumbilNo ratings yet
- Chapter 21 Antidepressant AgentsDocument4 pagesChapter 21 Antidepressant AgentsNicolle Lisay IlaganNo ratings yet
- Personality Dis PSTDocument79 pagesPersonality Dis PSTMonika JosephNo ratings yet
- Chapter 51 - Diuretic AgentsDocument11 pagesChapter 51 - Diuretic AgentsJonathon100% (2)