You might also like
- 1updated List of Drug ControllerDocument2 pages1updated List of Drug Controllerrr48843100% (1)
- KSRTC TicketDocument2 pagesKSRTC Ticketrr48843No ratings yet
- User Guide-9481903981Document19 pagesUser Guide-9481903981rr48843No ratings yet
- Meddra LLT Abbreviations / AcronymsDocument20 pagesMeddra LLT Abbreviations / Acronymsrr48843No ratings yet
- CROs in IndiaDocument6 pagesCROs in IndiaSivaNo ratings yet
- Pediatric Term List 16-1Document12 pagesPediatric Term List 16-1rr48843No ratings yet
- Med DRADocument3 pagesMed DRArr48843No ratings yet
- 114 Handy Formulae For Quantitative Aptitude ProblemsDocument12 pages114 Handy Formulae For Quantitative Aptitude ProblemsRaju.Konduru91% (69)
- User Guide-9481903981Document19 pagesUser Guide-9481903981rr48843No ratings yet
- Gender Term List 16-1Document30 pagesGender Term List 16-1rr48843No ratings yet
- Eu, Us and Indian Patent SystemDocument12 pagesEu, Us and Indian Patent Systemrr48843No ratings yet
- IndianJPharmacol4313-2929898 004849Document3 pagesIndianJPharmacol4313-2929898 004849rr48843No ratings yet
- MedDRA Pediatric Adverse Events List Uses and DevelopmentDocument2 pagesMedDRA Pediatric Adverse Events List Uses and Developmentrr48843No ratings yet
- Clinical Study Design GuidelinesDocument23 pagesClinical Study Design Guidelinesrr48843No ratings yet
- MedDRA LLT Abbreviations GuideDocument20 pagesMedDRA LLT Abbreviations Guiderr48843No ratings yet
- IndianJPharmacol393124-3017617 005017Document5 pagesIndianJPharmacol393124-3017617 005017rr48843No ratings yet
- IndianJPsycholMed332153-2605683 004325Document5 pagesIndianJPsycholMed332153-2605683 004325rr48843No ratings yet
- Pharmacovigilance in Teaching Hospital PDFDocument4 pagesPharmacovigilance in Teaching Hospital PDFrr48843No ratings yet
- IndianJPharmacol442257-1466766 040427Document4 pagesIndianJPharmacol442257-1466766 040427rr48843No ratings yet
- Natinal Pharmacovigilance ProgramDocument1 pageNatinal Pharmacovigilance Programrr48843No ratings yet
- IndianJPharmacol40137-144257 040025Document5 pagesIndianJPharmacol40137-144257 040025rr48843No ratings yet
- Challenges in Pharmacovigilance: EditorialDocument1 pageChallenges in Pharmacovigilance: Editorialrr48843No ratings yet
- IndianJPharmacol40728-3361566 005601Document4 pagesIndianJPharmacol40728-3361566 005601rr48843No ratings yet
- IndianJPharmacol393124-3017617 005017Document5 pagesIndianJPharmacol393124-3017617 005017rr48843No ratings yet
- Sakshi Education Website OverviewDocument2 pagesSakshi Education Website Overviewrr48843No ratings yet
- B ( Ýl (Ç Ólôœæ Ð) L$ ( Ð) Læý Y : SakshiDocument2 pagesB ( Ýl (Ç Ólôœæ Ð) L$ ( Ð) Læý Y : Sakshirr48843No ratings yet
- Companies TaglinesDocument7 pagesCompanies Taglinesrr48843No ratings yet
- Terminology-Constitution PDFDocument3 pagesTerminology-Constitution PDFyounusbasha143No ratings yet
- Sakshieducation Learning ResourcesDocument11 pagesSakshieducation Learning Resourcesrr48843No ratings yet
- (Ç Ç Èl ¿Ovøãmýs A Ô Ë$: SakshiDocument5 pages(Ç Ç Èl ¿Ovøãmýs A Ô Ë$: Sakshirr48843No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Investigation of Cyber CrimesDocument9 pagesInvestigation of Cyber CrimesHitesh BansalNo ratings yet
- Costco Case StudyDocument3 pagesCostco Case StudyMaong LakiNo ratings yet
- EDMOTO 4th TopicDocument24 pagesEDMOTO 4th TopicAngel Delos SantosNo ratings yet
- Invoice Inv0006: Er. Mohamed Irshadh P MDocument1 pageInvoice Inv0006: Er. Mohamed Irshadh P Mmanoj100% (1)
- Mariam Kairuz property dispute caseDocument7 pagesMariam Kairuz property dispute caseReginald Matt Aquino SantiagoNo ratings yet
- Master Your FinancesDocument15 pagesMaster Your FinancesBrendan GirdwoodNo ratings yet
- M8 UTS A. Sexual SelfDocument10 pagesM8 UTS A. Sexual SelfAnon UnoNo ratings yet
- Once in his Orient: Le Corbusier and the intoxication of colourDocument4 pagesOnce in his Orient: Le Corbusier and the intoxication of coloursurajNo ratings yet
- HLT42707 Certificate IV in Aromatherapy: Packaging RulesDocument2 pagesHLT42707 Certificate IV in Aromatherapy: Packaging RulesNilamdeen Mohamed ZamilNo ratings yet
- Oilwell Fishing Operations Tools and TechniquesDocument126 pagesOilwell Fishing Operations Tools and Techniqueskevin100% (2)
- Healthy Kitchen Shortcuts: Printable PackDocument12 pagesHealthy Kitchen Shortcuts: Printable PackAndre3893No ratings yet
- MadBeard Fillable Character Sheet v1.12Document4 pagesMadBeard Fillable Character Sheet v1.12DiononNo ratings yet
- The Wavy Tunnel: Trade Management Jody SamuelsDocument40 pagesThe Wavy Tunnel: Trade Management Jody SamuelsPeter Nguyen100% (1)
- Bajaj Allianz General Insurance Company LimitedDocument9 pagesBajaj Allianz General Insurance Company LimitedNaresh ChanchadNo ratings yet
- Latest Ku ReportDocument29 pagesLatest Ku Reportsujeet.jha.311No ratings yet
- English Course SyllabusDocument3 pagesEnglish Course Syllabusalea rainNo ratings yet
- Chapter 1Document30 pagesChapter 1Sneha AgarwalNo ratings yet
- Training of Local Government Personnel PHDocument5 pagesTraining of Local Government Personnel PHThea ConsNo ratings yet
- Perilaku Ramah Lingkungan Peserta Didik Sma Di Kota BandungDocument11 pagesPerilaku Ramah Lingkungan Peserta Didik Sma Di Kota Bandungnurulhafizhah01No ratings yet
- #1 HR Software in Sudan-Khartoum-Omdurman-Nyala-Port-Sudan - HR System - HR Company - HR SolutionDocument9 pages#1 HR Software in Sudan-Khartoum-Omdurman-Nyala-Port-Sudan - HR System - HR Company - HR SolutionHishamNo ratings yet
- Sewing Threads From Polyester Staple FibreDocument13 pagesSewing Threads From Polyester Staple FibreganeshaniitdNo ratings yet
- Colégio XIX de Março 2a Prova Substitutiva de InglêsDocument5 pagesColégio XIX de Março 2a Prova Substitutiva de InglêsCaio SenaNo ratings yet
- LS1 Eng. Modules With Worksheets (Figure of Speech)Document14 pagesLS1 Eng. Modules With Worksheets (Figure of Speech)Bong CardonaNo ratings yet
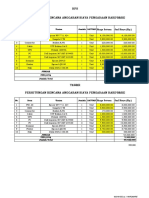
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDocument2 pagesHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriNo ratings yet
- Supplier of PesticidesDocument2 pagesSupplier of PesticidestusharNo ratings yet
- Adjusted School Reading Program of Buneg EsDocument7 pagesAdjusted School Reading Program of Buneg EsGener Taña AntonioNo ratings yet
- Line GraphDocument13 pagesLine GraphMikelAgberoNo ratings yet
- Whois contact details list with domainsDocument35 pagesWhois contact details list with domainsPrakash NNo ratings yet
- Bondor MultiDocument8 pagesBondor MultiPria UtamaNo ratings yet
- Individual Assessment Forms1Document9 pagesIndividual Assessment Forms1Maria Ivz ElborNo ratings yet