You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Annexure 2.3Document64 pagesAnnexure 2.3Siva Sankar ThungaNo ratings yet
- Chapter 12 - Auditing Inventories and Cost of Goods SoldDocument30 pagesChapter 12 - Auditing Inventories and Cost of Goods SoldJekNo ratings yet
- Overtime Pay-DOLEDocument1 pageOvertime Pay-DOLEJun CanilloNo ratings yet
- Ulangan SMSTR 1Document2 pagesUlangan SMSTR 1obito 22No ratings yet
- New Roma Communities in England:: Strategic Guide For Directors and Senior ManagementDocument28 pagesNew Roma Communities in England:: Strategic Guide For Directors and Senior ManagementLucie FremlovaNo ratings yet
- Bianca TimelineDocument4 pagesBianca TimelineNix RobertsNo ratings yet
- Food 8 - Part 2Document7 pagesFood 8 - Part 2Mónica MaiaNo ratings yet
- PMDT Product and SolutionDocument4 pagesPMDT Product and Solutionduong phamNo ratings yet
- Hertz Booster CompressorDocument4 pagesHertz Booster CompressorNaDeem NmsNo ratings yet
- Top 10 Solutions to Cut Poverty and Grow the Middle ClassDocument19 pagesTop 10 Solutions to Cut Poverty and Grow the Middle ClassLeilaAviorFernandezNo ratings yet
- TE27/32 Converter/Transmission Oil System SpecsDocument7 pagesTE27/32 Converter/Transmission Oil System SpecsGabrielNo ratings yet
- Ecological Solid Waste Management Survey at Barangay 41 BogtongDocument3 pagesEcological Solid Waste Management Survey at Barangay 41 BogtongRab Baloloy100% (1)
- ChoiDocument19 pagesChoiLuciana RafaelNo ratings yet
- Seom Clinical Guideline Ovarian Cancer 2020Document8 pagesSeom Clinical Guideline Ovarian Cancer 2020Romina DatuNo ratings yet
- Souldrama: A New Model For Putting The Twelve Steps Into ActionDocument3 pagesSouldrama: A New Model For Putting The Twelve Steps Into ActionedyyantoNo ratings yet
- Selected Answers For Exercises: Product KG Waste KG EDocument7 pagesSelected Answers For Exercises: Product KG Waste KG EkeatyNo ratings yet
- Centrifugal PumpDocument36 pagesCentrifugal PumpshubhamNo ratings yet
- GeneralChemistry1 q1 Mod3of8 Simple Seperation Techniques v2Document19 pagesGeneralChemistry1 q1 Mod3of8 Simple Seperation Techniques v2ALDRIN OBIASNo ratings yet
- Product CatalogDocument68 pagesProduct CatalogmunhNo ratings yet
- DR R K SharmaDocument375 pagesDR R K SharmaAparna DeviNo ratings yet
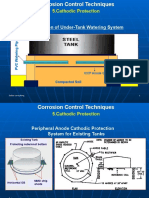
- Installation of Under-Tank Watering System: 5.cathodic ProtectionDocument35 pagesInstallation of Under-Tank Watering System: 5.cathodic ProtectionyouplaiNo ratings yet
- CHCDIV001 Work With Diverse People: Student Questions Case Study/ Scenarios Observations Oral Questions OtherDocument14 pagesCHCDIV001 Work With Diverse People: Student Questions Case Study/ Scenarios Observations Oral Questions OtherHardeep kaur0% (1)
- Utkarsha Ramteke - PGDM Candidate at IIM TrichyDocument1 pageUtkarsha Ramteke - PGDM Candidate at IIM TrichyyyyNo ratings yet
- Is The 'Next Friend' The Best FriendDocument5 pagesIs The 'Next Friend' The Best Friendarushi agarwalNo ratings yet
- Master Budget: Sales ForecastDocument61 pagesMaster Budget: Sales ForecastLay TekchhayNo ratings yet
- Pengendalian TYLCVDocument24 pagesPengendalian TYLCVMichael DeoNo ratings yet
- Motor Octane Number of Spark-Ignition Engine Fuel: Standard Test Method ForDocument56 pagesMotor Octane Number of Spark-Ignition Engine Fuel: Standard Test Method ForAMANDA BARRERA100% (1)
- ALS A&E REVIEWER: SCIENCE – ELEMENTARYDocument4 pagesALS A&E REVIEWER: SCIENCE – ELEMENTARYHorts JessaNo ratings yet
- The Play - Hansel and GretelDocument15 pagesThe Play - Hansel and Gretelidiomasnebrija100% (3)
- A Nursing Care Plan Presented To The Faculty of The Nursing DepartmentDocument8 pagesA Nursing Care Plan Presented To The Faculty of The Nursing DepartmentAlexandrea MayNo ratings yet