You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hema I Chapter 5 - SmearDocument36 pagesHema I Chapter 5 - SmearTesfaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Facts Statistics Awareness Video Clip Related Topics Citation Discussion PrintDocument6 pagesFacts Statistics Awareness Video Clip Related Topics Citation Discussion PrintprasadNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- HistologyDocument77 pagesHistologyRahul0% (1)
- 1-Blood Pressure Palpatory MethodDocument2 pages1-Blood Pressure Palpatory MethodUsama100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Hematology Chap 12Document30 pagesHematology Chap 12Eyasu demsewNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Whole Milk Powder (WMP), International Market - Western EuropeDocument3 pagesWhole Milk Powder (WMP), International Market - Western EuropeGEMINI MARIE ARROJONo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Coagulation Cascade 3 - Halflives of The Coagulation FactorsDocument1 pageCoagulation Cascade 3 - Halflives of The Coagulation FactorsAbdur rehmanNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- PediatricsDocument33 pagesPediatricsnageshwarioshNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- ASTM 71830-97 - Standard Practice For Selection of Blood For in Vitro Evaluation of Blood PumpsDocument2 pagesASTM 71830-97 - Standard Practice For Selection of Blood For in Vitro Evaluation of Blood PumpsJoãoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Order of DrawDocument8 pagesOrder of DrawVincent ReyesNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Vlaar2021 Article TransfusionStrategiesInBleedinDocument25 pagesVlaar2021 Article TransfusionStrategiesInBleedinRaul DoctoNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elution and Adsorption TechniquesDocument23 pagesElution and Adsorption TechniquesBromance H.No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- l5 Hemolytic Disease of Newborn HDNDocument26 pagesl5 Hemolytic Disease of Newborn HDNmaher Haji officialNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Uniplastin IfuDocument2 pagesUniplastin IfuTapabrata MaityNo ratings yet
- 5BIOM007W Applied Pathobiology 2017Document3 pages5BIOM007W Applied Pathobiology 2017Alhassan ColleyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Coagulation disorders-MS1Document46 pagesCoagulation disorders-MS1Chamika Huruggamuwa100% (1)
- ForensicSerology (Student Version)Document19 pagesForensicSerology (Student Version)Normalyn Andres MacaysaNo ratings yet
- Blood and Bloodstains: Harry Danny L. Aspillaga Instructor Forensic Chemistry and ToxicologyDocument50 pagesBlood and Bloodstains: Harry Danny L. Aspillaga Instructor Forensic Chemistry and ToxicologyHarry Danny AspillagaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Phlebotomy NHA ReviewDocument6 pagesPhlebotomy NHA ReviewJuju Jing100% (4)
- Booklet 2 Donador de SangreDocument16 pagesBooklet 2 Donador de SangreKatherine QuinteroNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
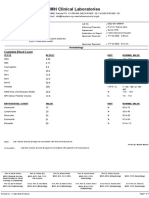
- FMH Clinical Laboratories: Complete Blood CountDocument1 pageFMH Clinical Laboratories: Complete Blood CountZahid AliNo ratings yet
- Bbms Program Internship (INT 510) Daily Internship LogDocument3 pagesBbms Program Internship (INT 510) Daily Internship LogGhina YazbekNo ratings yet
- ID Efektivitas Senam Jantung Sehat TerhadapDocument7 pagesID Efektivitas Senam Jantung Sehat TerhadapAisyah SyahidahNo ratings yet
- Comprehensive LectureDocument87 pagesComprehensive LectureDeniel Busi100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Blood Transfusion SLPDocument10 pagesBlood Transfusion SLPLovesehun OhNo ratings yet
- Hemostasis: Mechanisms of Blood CoagulationDocument2 pagesHemostasis: Mechanisms of Blood CoagulationAshish SrivastavaNo ratings yet
- Laporan IPEDocument15 pagesLaporan IPERidha FadhilaNo ratings yet
- BONAVERA CountDocument15 pagesBONAVERA CountpsychejaneNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Blood Group Systems ISBTDocument25 pagesBlood Group Systems ISBTkusumahpratiwi100% (1)
- 10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)Document45 pages10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)MUHAMMAD BAGIR ALJUFRINo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)