You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Pdhpe Notes FullDocument79 pagesPdhpe Notes FullFarhad HakimiNo ratings yet
- Mary Mount School of Koronadal Incorporated: Clinic CalendarDocument2 pagesMary Mount School of Koronadal Incorporated: Clinic CalendarTeàcher Peach100% (2)
- Mission Indradhanush: Submitted By-Jayesh Agrawal Mba-Rural Development Semester-IstDocument20 pagesMission Indradhanush: Submitted By-Jayesh Agrawal Mba-Rural Development Semester-IstJayeshAgrawalNo ratings yet
- Working PhaseDocument7 pagesWorking PhaseSytrose MoralesNo ratings yet
- OAEM 22802 Validation of The Thorax Trauma Severity Score For Mortality 082211Document5 pagesOAEM 22802 Validation of The Thorax Trauma Severity Score For Mortality 082211MedischManNo ratings yet
- Atr 01 54Document4 pagesAtr 01 54MedischManNo ratings yet
- Sub HaniDocument4 pagesSub HaniMedischManNo ratings yet
- The Prognostic Importance of Trauma Scoring SystemsDocument6 pagesThe Prognostic Importance of Trauma Scoring SystemsMedischManNo ratings yet
- Atr 01 54Document4 pagesAtr 01 54MedischManNo ratings yet
- NHO Medical Abbreviations BookletDocument54 pagesNHO Medical Abbreviations BookletffsdfsfdftrertNo ratings yet
- Perdarahan ObstetryDocument43 pagesPerdarahan ObstetryPutri EffendyNo ratings yet
- DR Moshiri - Class II Correction by Leveraging Molar Rotation - 2Document4 pagesDR Moshiri - Class II Correction by Leveraging Molar Rotation - 2Enea NastriNo ratings yet
- M. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingDocument11 pagesM. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingMallika JoonNo ratings yet
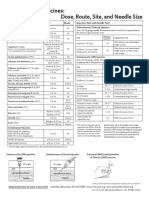
- Injection Site and Needle Size Vaccine Dose RouteDocument1 pageInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNo ratings yet
- Bev Johnson, Et AlDocument34 pagesBev Johnson, Et AlNanda Trisna OliviaNo ratings yet
- APPOINTMENTDocument1 pageAPPOINTMENTNur Hazimah50% (2)
- Healthcare For The ImmigrantDocument7 pagesHealthcare For The Immigrantursula56No ratings yet
- Reflection PaperDocument2 pagesReflection PaperSylvanus Rein LangreoNo ratings yet
- Cervical Insufficiency + Cord PresentationDocument2 pagesCervical Insufficiency + Cord PresentationMSNo ratings yet
- COVIDDocument13 pagesCOVIDStephen RomeroNo ratings yet
- Mortalidad Adultos MundoDocument86 pagesMortalidad Adultos MundoJacob DavisNo ratings yet
- New Roles Pharmacists: Value-Based Pay Creates OpportunitiesDocument33 pagesNew Roles Pharmacists: Value-Based Pay Creates OpportunitiesAnonymous EAPbx6No ratings yet
- PE and Health: Quarter 2 Module 8 Organizing A Dance EventDocument6 pagesPE and Health: Quarter 2 Module 8 Organizing A Dance EventMary Joy Cejalbo100% (1)
- 2 - Labor and DystociaDocument8 pages2 - Labor and DystociaJC GoodLifeNo ratings yet
- Community Medicine 2022Document8 pagesCommunity Medicine 2022Ashirwad DadeiaNo ratings yet
- Prevention of Postpartum Psychosis PDFDocument7 pagesPrevention of Postpartum Psychosis PDFAjengNo ratings yet
- Luis Andres Arcos Montoya 2014Document11 pagesLuis Andres Arcos Montoya 2014luisandresarcosNo ratings yet
- Funda Lab - Prelim ReviewerDocument16 pagesFunda Lab - Prelim ReviewerNikoruNo ratings yet
- Causes of Death in HIV-infected Persons Who Have Tuberculosis, ThailandDocument7 pagesCauses of Death in HIV-infected Persons Who Have Tuberculosis, Thailandfaradila aninda raesaNo ratings yet
- Mayo Clinic Authorizations and Service TermsDocument1 pageMayo Clinic Authorizations and Service TermsjamesjohnsonamazonprimeNo ratings yet
- Radiofrequency AblationDocument7 pagesRadiofrequency AblationRohit singhNo ratings yet
- Carillo vs. PeopleDocument6 pagesCarillo vs. PeopleJenny ButacanNo ratings yet
- Patient Identity PolicyDocument6 pagesPatient Identity PolicyAnnie JonesNo ratings yet
- Case Study: Epidemiology LaboratoryDocument5 pagesCase Study: Epidemiology LaboratoryDonna IlarNo ratings yet
- Bwdi DR, Chemist&Stp Final ListDocument226 pagesBwdi DR, Chemist&Stp Final ListzaheerbcNo ratings yet