You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Uro ChordataDocument4 pagesUro ChordataSana SiddiqueNo ratings yet
- The Conceptualization of Emotions Across Cultures: A Model Based On Interoceptive NeuroscienceDocument14 pagesThe Conceptualization of Emotions Across Cultures: A Model Based On Interoceptive NeurosciencepartoNo ratings yet
- DNA Translation Written ReportDocument5 pagesDNA Translation Written ReportHerlene SeeNo ratings yet
- ABO Incompatibility in NewbornsDocument4 pagesABO Incompatibility in NewbornsNollen LaquianNo ratings yet
- Growth and DevelopmentDocument21 pagesGrowth and DevelopmentKarl Sean UbinaNo ratings yet
- Case StudyDocument6 pagesCase StudySarah McKayNo ratings yet
- 10th SCERT KeralaDocument72 pages10th SCERT KeralaArun KNo ratings yet
- Anaphy (Intro - Skeletal System) ReviewerDocument34 pagesAnaphy (Intro - Skeletal System) ReviewerYanna G.No ratings yet
- Veta 3 - Datasheet - ENG - 20210315Document2 pagesVeta 3 - Datasheet - ENG - 20210315JuanNo ratings yet
- Correlation of Red Blood Cell Distribution Width (RDW) and Haemoglobin A1C (Hba1C) Levels in Diabetic IndividualsDocument13 pagesCorrelation of Red Blood Cell Distribution Width (RDW) and Haemoglobin A1C (Hba1C) Levels in Diabetic IndividualsfachrurNo ratings yet
- Importance of Anaerobic Glycolysis & Stiffness in SprintsDocument7 pagesImportance of Anaerobic Glycolysis & Stiffness in SprintsAltec AlsingNo ratings yet
- g12 Bone Grafts Subs JTG Rev 10 17 10Document57 pagesg12 Bone Grafts Subs JTG Rev 10 17 10Tudor RalucaNo ratings yet
- The Problem and Its BackgroundDocument43 pagesThe Problem and Its BackgroundkjjkjkljkjjklNo ratings yet
- How to Dilute Blood and Count White Blood CellsDocument2 pagesHow to Dilute Blood and Count White Blood CellsAlfred ChowNo ratings yet
- Chapter 013Document4 pagesChapter 013Nusa Koj100% (1)
- Fungsi Otot-OtotDocument32 pagesFungsi Otot-OtothansenpanjaitanNo ratings yet
- Jeffrey SatinoverDocument7 pagesJeffrey SatinoverlooiiiiisNo ratings yet
- Anatomy, Lecture 7, Thorax & Superior Mediastinum (Lecture NOtes)Document13 pagesAnatomy, Lecture 7, Thorax & Superior Mediastinum (Lecture NOtes)Ali Al-QudsiNo ratings yet
- Broncho DilatorsDocument53 pagesBroncho DilatorsDocRNNo ratings yet
- PNTD 0005534 s001Document22 pagesPNTD 0005534 s001Paolo VidalNo ratings yet
- CBSE Class 9 Science Worksheet - Tissues AnimalsDocument2 pagesCBSE Class 9 Science Worksheet - Tissues Animalsanimetaha353No ratings yet
- Review of Placenta DeliveryDocument3 pagesReview of Placenta DeliverygitapramodhaNo ratings yet
- Animals Have Basic NeedsDocument24 pagesAnimals Have Basic NeedsNarendran SubramaniamNo ratings yet
- Glikogenesis Dan GlikogenolisisDocument23 pagesGlikogenesis Dan GlikogenolisisKinarNo ratings yet
- PB - Interpreting An Investigation of Plant Hormones QPDocument6 pagesPB - Interpreting An Investigation of Plant Hormones QPRutba SafdarNo ratings yet
- Article - ECG Vs MCGDocument7 pagesArticle - ECG Vs MCGpaul_calburean7899No ratings yet
- Intestinal Obstruction: A Report by C2Document22 pagesIntestinal Obstruction: A Report by C2Teanu Jose Gabrillo TamayoNo ratings yet
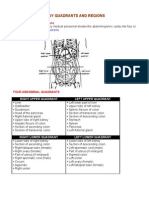
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- Cell Biology and Molecular ScienceDocument139 pagesCell Biology and Molecular ScienceLike GhazalNo ratings yet
- KIT CD117 A Review On Expression in Normal and Neoplastic TissuesDocument16 pagesKIT CD117 A Review On Expression in Normal and Neoplastic TissuesVlado VladNo ratings yet