You might also like
- 14 - Perawatan Endodontic Gigi Molar Dengan Perforasi BifurkasiDocument5 pages14 - Perawatan Endodontic Gigi Molar Dengan Perforasi Bifurkasisarah hanifahNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFZaenuriNo ratings yet
- Preparasi Gigi AbutmentDocument15 pagesPreparasi Gigi AbutmentFransiskus Xaverius DoddieNo ratings yet
- Caries ProfundaDocument8 pagesCaries ProfundacyntiamalikfaNo ratings yet
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Case Report Fissure SealantDocument8 pagesCase Report Fissure SealantrespikNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Fish Bone Analysis of Self-Medication in IndonesiaDocument6 pagesFish Bone Analysis of Self-Medication in IndonesiaDedy MahendraNo ratings yet
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocument6 pagesClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaNo ratings yet
- Modified Bluegrass Appliance PDFDocument4 pagesModified Bluegrass Appliance PDFRenieKumalaNo ratings yet
- Developmental DefectsDocument29 pagesDevelopmental DefectsPrince AhmedNo ratings yet
- FINAL SplintingDocument46 pagesFINAL SplintingDilmohit SinghNo ratings yet
- SSCDocument10 pagesSSCYanuar MegaNo ratings yet
- Hidden CariesDocument10 pagesHidden Cariesyenni_windasariNo ratings yet
- Cara Penggunaaan DevitalDocument2 pagesCara Penggunaaan DevitalKrisbudiSetyawanNo ratings yet
- SOCA Blok 12Document21 pagesSOCA Blok 12safiraNo ratings yet
- Analisa Lundstrom Rahang AtasDocument1 pageAnalisa Lundstrom Rahang AtasmfahrizaNo ratings yet
- Penggunaan Polyethylene Fiber-Reinforced Composite Resin Sebagai Short Post Dan Inti Pada Gigi Anterior Sulung Dengan Karies Yang Luas Laporan KasusDocument14 pagesPenggunaan Polyethylene Fiber-Reinforced Composite Resin Sebagai Short Post Dan Inti Pada Gigi Anterior Sulung Dengan Karies Yang Luas Laporan Kasusfebriani serojaNo ratings yet
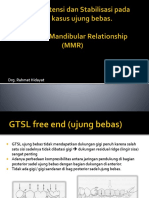
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 pagesDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarNo ratings yet
- Formato Cambra 6 Años en AdelanteDocument2 pagesFormato Cambra 6 Años en AdelanteSandra GutiérrezNo ratings yet
- Jurnal Mounting Articulator PDFDocument6 pagesJurnal Mounting Articulator PDFKhaleda ShafiraNo ratings yet
- Provisional Splinting 2013Document87 pagesProvisional Splinting 2013felicedaNo ratings yet
- Space Maintainers: A Review: International Journal of Medical and Health ResearchDocument4 pagesSpace Maintainers: A Review: International Journal of Medical and Health Researchpaper kitaNo ratings yet
- Space RegainerDocument7 pagesSpace RegainerdelfNo ratings yet
- Fissure TongueDocument2 pagesFissure Tonguebundahara zoomNo ratings yet
- Guided Tissue RegenerationDocument4 pagesGuided Tissue RegenerationNicoleta MarcuNo ratings yet
- Splinting 150507152946 Lva1 App6891 PDFDocument92 pagesSplinting 150507152946 Lva1 App6891 PDFade ismailNo ratings yet
- ADA Caries Risk Assessmento Mayores 6Document2 pagesADA Caries Risk Assessmento Mayores 6Catalina Cané Muñoz SilvaNo ratings yet
- Ellis ClassificationDocument1 pageEllis ClassificationBrigs De GuzmanNo ratings yet
- Brochure-Gc Fuji ViiDocument16 pagesBrochure-Gc Fuji ViiZulfahmi NurdinNo ratings yet
- Presentation1 PdiDocument51 pagesPresentation1 PdiAisha samreenNo ratings yet
- Chronic Hyperplastic PulpitisDocument30 pagesChronic Hyperplastic PulpitisGlory Pohan67% (3)
- Management of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryDocument4 pagesManagement of Pericoronitis of Newly-Erupted Permanent Tooth Using ElectrosurgeryLatifa Hanif ZuhriNo ratings yet
- Prostho Vi - Slides 5 - Occlusal - ConsiderationsDocument83 pagesProstho Vi - Slides 5 - Occlusal - Considerationsبراءة أحمد السلاماتNo ratings yet
- Enamel Acid Etching - A ReviewDocument8 pagesEnamel Acid Etching - A ReviewSiddharth NairNo ratings yet
- Clinical Evaluation Between Zirconia Crowns and Stainless Steel Crowns in Primary Molars TeethDocument7 pagesClinical Evaluation Between Zirconia Crowns and Stainless Steel Crowns in Primary Molars TeethninisskyNo ratings yet
- Hemiseksi Akar Distal Molar Kedua Rahang BawahDocument5 pagesHemiseksi Akar Distal Molar Kedua Rahang BawahAhmad Willy AntonNo ratings yet
- Case Report - Complete Denture - 2Document4 pagesCase Report - Complete Denture - 2Astri Ggamjong Xiao LuNo ratings yet
- Extrinsic Stains and Deposits On TeethDocument9 pagesExtrinsic Stains and Deposits On TeethFredie Jun Onio100% (1)
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocument132 pagesComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanNo ratings yet
- Restoring Posterior Tooth with Semidirect TechniqueDocument4 pagesRestoring Posterior Tooth with Semidirect Techniquemartariwansyah100% (1)
- Adhesive BridgesDocument9 pagesAdhesive BridgesShilpa ShrivastavaNo ratings yet
- Polishing Amalgam RestorationsDocument39 pagesPolishing Amalgam RestorationsMuad AbulohomNo ratings yet
- Cu Sil DenturesDocument6 pagesCu Sil Denturessiddu76No ratings yet
- Kuliah Glass Ionomer CementDocument40 pagesKuliah Glass Ionomer CementMaika RatriNo ratings yet
- Acc Pain FauziDocument8 pagesAcc Pain FauziMuchlis Fauzi ENo ratings yet
- Curve of SpeeDocument7 pagesCurve of SpeeKorina CallerosNo ratings yet
- Causes and prevention of ledging and blockages in root canalsDocument19 pagesCauses and prevention of ledging and blockages in root canalsBunga Erlita RosaliaNo ratings yet
- Pdi Partial EdentulismDocument67 pagesPdi Partial EdentulismAnkeeta ShuklaNo ratings yet
- Endocrowns A Systematic ReviewDocument17 pagesEndocrowns A Systematic Reviewaulia lubisNo ratings yet
- Klasifikasi AramanyDocument7 pagesKlasifikasi AramanyThio ZhuNo ratings yet
- Unilateral Leukoedema CaseDocument2 pagesUnilateral Leukoedema CaseBramita Beta ArnandaNo ratings yet
- Abses IntraoralDocument19 pagesAbses IntraoralTitis LaraswatiNo ratings yet
- A To Z Orthodontics Vol 24 Orthodontic Practical NotesDocument83 pagesA To Z Orthodontics Vol 24 Orthodontic Practical Notesdent in dentist100% (2)
- KRS 03111402063 Semester 4 2012-2013Document4 pagesKRS 03111402063 Semester 4 2012-2013Indah SimamoraNo ratings yet
- Pathology of Oral Cavity ManifestationsDocument9 pagesPathology of Oral Cavity Manifestationscreature123No ratings yet
- PericoronitisAugSept09 2Document10 pagesPericoronitisAugSept09 2dodol_cowboyNo ratings yet
- Alamat Korespondensi: Bagian Prostodonsia Fakultas Kedokteran Gigi Universitas Gadjah Mada Indonesian Journal of Dentistry 2008; 15 (3):187-191 Fakultas Kedokteran Gigi http//www.fkg.ui.edu Universitas Indonesia ISSN 1693-9697 PENGARUH EKSTRAK GRAPTOPHYLLUM PICTUM TERHADAP PERTUMBUHAN CANDIDA ALBICANS PADA PLAT GIGI TIRUAN RESIN AKRILIK Endang Wahyuningtyas Bagian Prostodonsia Fakultas Kedokteran Gigi Universitas Gadjah Mada Abstract Graptophyllum pictum (Daun ungu) is one of the traditional plants in Indonesia. Graptophyllum pictum composition is flavonoid, Flavonoid has an antimicrobial effect. The purpose of this study is to find the effect of Graptophyllum pictum extract prevent the growth of Candida albicans on acrylic resin denture plate. The research was done plaque smear which Candida albicans adhered at the patient denture, then it was cultured and Candida albicans growth was cultivated. The research was done by using 40 samples. The samples were heat cured aDocument5 pagesAlamat Korespondensi: Bagian Prostodonsia Fakultas Kedokteran Gigi Universitas Gadjah Mada Indonesian Journal of Dentistry 2008; 15 (3):187-191 Fakultas Kedokteran Gigi http//www.fkg.ui.edu Universitas Indonesia ISSN 1693-9697 PENGARUH EKSTRAK GRAPTOPHYLLUM PICTUM TERHADAP PERTUMBUHAN CANDIDA ALBICANS PADA PLAT GIGI TIRUAN RESIN AKRILIK Endang Wahyuningtyas Bagian Prostodonsia Fakultas Kedokteran Gigi Universitas Gadjah Mada Abstract Graptophyllum pictum (Daun ungu) is one of the traditional plants in Indonesia. Graptophyllum pictum composition is flavonoid, Flavonoid has an antimicrobial effect. The purpose of this study is to find the effect of Graptophyllum pictum extract prevent the growth of Candida albicans on acrylic resin denture plate. The research was done plaque smear which Candida albicans adhered at the patient denture, then it was cultured and Candida albicans growth was cultivated. The research was done by using 40 samples. The samples were heat cured aRiesky SharastitiNo ratings yet
- Pathogenesis Gingivitis Young and AdultDocument12 pagesPathogenesis Gingivitis Young and AdultIndah SimamoraNo ratings yet
- 1572-3faktor-Faktor Yang Berhubungan Dengan Praktik Penggunaan Masker Pada Pekerja Bagian Pencelupan BenangDocument8 pages1572-3faktor-Faktor Yang Berhubungan Dengan Praktik Penggunaan Masker Pada Pekerja Bagian Pencelupan BenangIndah SimamoraNo ratings yet
- Young Practitioners Guide To PeriodontologyDocument36 pagesYoung Practitioners Guide To PeriodontologyAndrea Law100% (3)
- Periodontology MCQDocument12 pagesPeriodontology MCQIndah Simamora67% (3)
- Murray AJD June 2006 WebDocument7 pagesMurray AJD June 2006 WebIndah SimamoraNo ratings yet
- Phototoxic Effect of Non-Coherent Light On Perio-Pathogens: Dentistry/Oral MedicineDocument3 pagesPhototoxic Effect of Non-Coherent Light On Perio-Pathogens: Dentistry/Oral MedicineIndah SimamoraNo ratings yet
- Natural Preservatives OriginalDocument33 pagesNatural Preservatives OriginalSudip GhoshNo ratings yet
- 14 13 1 PB PDFDocument9 pages14 13 1 PB PDFRizki PuspitasariNo ratings yet
- Simple Essential Oil Remedies To The Most Common AilmentsDocument4 pagesSimple Essential Oil Remedies To The Most Common AilmentsIndah SimamoraNo ratings yet
- Susceptibilities Candida To Antifungal AgentsDocument8 pagesSusceptibilities Candida To Antifungal AgentsIndah SimamoraNo ratings yet
- 'The Flavor and Fragrance High Production Volume ConsortiaDocument55 pages'The Flavor and Fragrance High Production Volume ConsortiaIndah SimamoraNo ratings yet
- Chi Square 12Document15 pagesChi Square 12devilsayangNo ratings yet
- 71073438Document5 pages71073438Indah SimamoraNo ratings yet
- Whisper Flo XF 3 PhaseDocument16 pagesWhisper Flo XF 3 Phasehargote_2No ratings yet
- IoT BASED HEALTH MONITORING SYSTEMDocument18 pagesIoT BASED HEALTH MONITORING SYSTEMArunkumar Kuti100% (2)
- Mercedes BenzDocument56 pagesMercedes BenzRoland Joldis100% (1)
- RUJUKANDocument3 pagesRUJUKANMaryTibanNo ratings yet
- The Berkeley Review: MCAT Chemistry Atomic Theory PracticeDocument37 pagesThe Berkeley Review: MCAT Chemistry Atomic Theory Practicerenjade1516No ratings yet
- Unit 1 TQM NotesDocument26 pagesUnit 1 TQM NotesHarishNo ratings yet
- The Impact of School Facilities On The Learning EnvironmentDocument174 pagesThe Impact of School Facilities On The Learning EnvironmentEnrry Sebastian71% (31)
- IGCSE Chemistry Section 5 Lesson 3Document43 pagesIGCSE Chemistry Section 5 Lesson 3Bhawana SinghNo ratings yet
- MODULE+4+ +Continuous+Probability+Distributions+2022+Document41 pagesMODULE+4+ +Continuous+Probability+Distributions+2022+Hemis ResdNo ratings yet
- Final Thesis Report YacobDocument114 pagesFinal Thesis Report YacobAddis GetahunNo ratings yet
- Cold Rolled Steel Sections - Specification: Kenya StandardDocument21 pagesCold Rolled Steel Sections - Specification: Kenya StandardPEng. Tech. Alvince KoreroNo ratings yet
- ISO 9001:2015 Explained, Fourth Edition GuideDocument3 pagesISO 9001:2015 Explained, Fourth Edition GuideiresendizNo ratings yet
- RACI Matrix: Phase 1 - Initiaton/Set UpDocument3 pagesRACI Matrix: Phase 1 - Initiaton/Set UpHarshpreet BhatiaNo ratings yet
- How Psychology Has Changed Over TimeDocument2 pagesHow Psychology Has Changed Over TimeMaedot HaddisNo ratings yet
- Experiences from OJT ImmersionDocument3 pagesExperiences from OJT ImmersionTrisha Camille OrtegaNo ratings yet
- Data Sheet: Experiment 5: Factors Affecting Reaction RateDocument4 pagesData Sheet: Experiment 5: Factors Affecting Reaction Ratesmuyet lêNo ratings yet
- DLL - The Firm and Its EnvironmentDocument5 pagesDLL - The Firm and Its Environmentfrances_peña_7100% (2)
- Analytical Approach To Estimate Feeder AccommodatiDocument16 pagesAnalytical Approach To Estimate Feeder AccommodatiCleberton ReizNo ratings yet
- Tension field beams: Aircraft wing spar analysisDocument19 pagesTension field beams: Aircraft wing spar analysisPrajeesh RajNo ratings yet
- Pita Cyrel R. Activity 7Document5 pagesPita Cyrel R. Activity 7Lucky Lynn AbreraNo ratings yet
- Sri S T Kalairaj, Chairman: Income Tax TaxesDocument3 pagesSri S T Kalairaj, Chairman: Income Tax TaxesvikramkkNo ratings yet
- Pre Job Hazard Analysis (PJHADocument2 pagesPre Job Hazard Analysis (PJHAjumaliNo ratings yet
- Coffee Table Book Design With Community ParticipationDocument12 pagesCoffee Table Book Design With Community ParticipationAJHSSR JournalNo ratings yet
- Clark DietrichDocument110 pagesClark Dietrichikirby77No ratings yet
- Yellowstone Food WebDocument4 pagesYellowstone Food WebAmsyidi AsmidaNo ratings yet
- MID TERM Question Paper SETTLEMENT PLANNING - SEC CDocument1 pageMID TERM Question Paper SETTLEMENT PLANNING - SEC CSHASHWAT GUPTANo ratings yet
- India Today 11-02-2019 PDFDocument85 pagesIndia Today 11-02-2019 PDFGNo ratings yet
- Logic and Set Theory PropositionDocument3 pagesLogic and Set Theory PropositionVince OjedaNo ratings yet
- Inside Animator PDFDocument484 pagesInside Animator PDFdonkey slapNo ratings yet
- Orc & Goblins VII - 2000pts - New ABDocument1 pageOrc & Goblins VII - 2000pts - New ABDave KnattNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)