You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Hugo German3months 2011Document139 pagesHugo German3months 2011Edvin Musi100% (1)
- 213 NnadDocument1 page213 NnadEdvin MusiNo ratings yet
- TL-WR941HP (Un) V1 UgDocument177 pagesTL-WR941HP (Un) V1 UgNico SilabanNo ratings yet
- TL-WR941HP (Un) V1 UgDocument177 pagesTL-WR941HP (Un) V1 UgNico SilabanNo ratings yet
- BettDocument2 pagesBettEdvin MusiNo ratings yet
- 3M 22Document9 pages3M 22Edvin MusiNo ratings yet
- Slovakia 14Document11 pagesSlovakia 14Edvin MusiNo ratings yet
- BettDocument2 pagesBettEdvin MusiNo ratings yet
- 3M 22Document9 pages3M 22Edvin MusiNo ratings yet
- 3M 22Document9 pages3M 22Edvin MusiNo ratings yet
- GSDocument3 pagesGSEdvin MusiNo ratings yet
- 11.in Flight HebrewDocument20 pages11.in Flight HebrewmaorumfernandesNo ratings yet
- GSDocument3 pagesGSEdvin MusiNo ratings yet
- 45manual m238 ProgramDocument230 pages45manual m238 ProgramEdvin MusiNo ratings yet
- Introduction To Industrial Control Networks: Brendan Galloway and Gerhard P. Hancke, Senior Member, IEEEDocument22 pagesIntroduction To Industrial Control Networks: Brendan Galloway and Gerhard P. Hancke, Senior Member, IEEEEdvin MusiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDocument2 pagesProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNo ratings yet
- Curriculum Vitae: Dr. Avinash K. Jangde - . - ., - . (A)Document5 pagesCurriculum Vitae: Dr. Avinash K. Jangde - . - ., - . (A)Mohammad TariqNo ratings yet
- ProspectusDocument156 pagesProspectusNareshNo ratings yet
- Maquet Meera BrochureDocument16 pagesMaquet Meera BrochureFeridun MADRANNo ratings yet
- Sources of Homeopathic DrugsDocument35 pagesSources of Homeopathic Drugsnadiida83% (6)
- Tissue TypingDocument4 pagesTissue TypingNoura Al-Hussainan100% (1)
- IMCI Chart BookletDocument66 pagesIMCI Chart Bookletnorwin_033875No ratings yet
- Current Management of LabourDocument48 pagesCurrent Management of Labourapi-3705046100% (4)
- Principle of Laser Application in Medicine & LASER SAFETY5Document62 pagesPrinciple of Laser Application in Medicine & LASER SAFETY5melisandrianaNo ratings yet
- Techniques For Parasite Egg Identification in Faecal SamplesDocument9 pagesTechniques For Parasite Egg Identification in Faecal SamplesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- Windy WigaDocument2 pagesWindy WigaWindy wigaNo ratings yet
- PBL 1 - Post Streptococcal Rheumatic Fever PolicyDocument8 pagesPBL 1 - Post Streptococcal Rheumatic Fever PolicyAinur AbdrakhmanovaNo ratings yet
- Item Balance Per Unit RPTDocument60 pagesItem Balance Per Unit RPTYogie 1290No ratings yet
- Rosen's Emergency Medicine Concepts and Clinical PracticeDocument15 pagesRosen's Emergency Medicine Concepts and Clinical PracticeMusdal RahmatNo ratings yet
- Philosophy of OcclusionDocument23 pagesPhilosophy of OcclusionAnil SukumaranNo ratings yet
- Ujian Akhir Semester Susulam Basic EnglishDocument15 pagesUjian Akhir Semester Susulam Basic EnglishNadia 13No ratings yet
- Anxiety Disorders BBDocument18 pagesAnxiety Disorders BBRyan Justin BoudreauxNo ratings yet
- Face PresentationDocument6 pagesFace PresentationNishaThakuriNo ratings yet
- Source: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical EthicsDocument67 pagesSource: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical Ethicsjamestery0% (1)
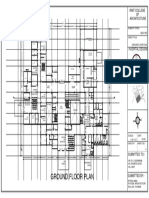
- Ground Floor Plan Sheet 2Document1 pageGround Floor Plan Sheet 2riteshNo ratings yet
- Tanzania STG 052013-Copy 1544379670122Document220 pagesTanzania STG 052013-Copy 1544379670122Waqar WikiNo ratings yet
- Impact of School Health Education Program On PersonalDocument4 pagesImpact of School Health Education Program On Personalaspiah mahmudNo ratings yet
- Sodium Chloride (Rock Salt) MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesSodium Chloride (Rock Salt) MSDS: Section 1: Chemical Product and Company IdentificationMohamed MaghawryNo ratings yet
- Love Pain e Book PDFDocument14 pagesLove Pain e Book PDFTina AnesNo ratings yet
- EndometriosisDocument153 pagesEndometriosisoannny8661No ratings yet
- 200 Terms & Definition From Pharmacology. WatermarkedDocument17 pages200 Terms & Definition From Pharmacology. Watermarkedsuresh adgaonkar100% (1)
- AlprazolamDocument10 pagesAlprazolamWen SilverNo ratings yet
- Crystal Aromatherapy Lesson 1Document9 pagesCrystal Aromatherapy Lesson 1crystals21No ratings yet
- 10 Hip Replacement SurgeryDocument13 pages10 Hip Replacement SurgeryDIA PHONG THANGNo ratings yet
- Medical Surgical Nursing ReviewDocument97 pagesMedical Surgical Nursing ReviewBernadeth Josefa BorelaNo ratings yet