You might also like
- Metro Quiz 2Document4 pagesMetro Quiz 2Jai O. VillaNo ratings yet
- NBME 5 - Block 1Document51 pagesNBME 5 - Block 1junkpyunjee993317No ratings yet
- 978190medicine5635856 PDFDocument18 pages978190medicine5635856 PDFMuhammad TariqNo ratings yet
- Primer 03a Enterobacteriase and Diarrhea PDFDocument4 pagesPrimer 03a Enterobacteriase and Diarrhea PDFJai O. VillaNo ratings yet
- Primer 07aaa Study GuidepdfDocument3 pagesPrimer 07aaa Study GuidepdfJai O. VillaNo ratings yet
- Sympathetics 07 A Study GuidepdfDocument3 pagesSympathetics 07 A Study GuidepdfJai O. VillaNo ratings yet
- 2013 FA Step 1 Errata Final 131231Document11 pages2013 FA Step 1 Errata Final 131231Jai O. VillaNo ratings yet
- FaqsDocument2 pagesFaqschaz1No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Understanding Ekgs A Practical Approach 4th Edition Ebook PDFDocument57 pagesUnderstanding Ekgs A Practical Approach 4th Edition Ebook PDFjessica.taylor655100% (38)
- ECGDocument154 pagesECGSandeep BansalNo ratings yet
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceBharathbushan V MandiriNo ratings yet
- Basic Life SupportDocument6 pagesBasic Life SupportRyan Mathew ScottNo ratings yet
- Congenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekDocument43 pagesCongenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekAdel HamzicNo ratings yet
- Cardiac Catheterization Knowledge & Skills ChecklistDocument6 pagesCardiac Catheterization Knowledge & Skills ChecklistnorthweststaffingNo ratings yet
- Drug-Eluting Balloon: New Tool in The BoxDocument8 pagesDrug-Eluting Balloon: New Tool in The BoxARUN KUMARNo ratings yet
- Infant Tachycardia ECG Differential DiagnosisDocument5 pagesInfant Tachycardia ECG Differential DiagnosisDeepak KumarNo ratings yet
- Evaluation of The R One Robotic System For Percutaneous Coronary Intervention THDocument11 pagesEvaluation of The R One Robotic System For Percutaneous Coronary Intervention THNeranga SamaratungeNo ratings yet
- A Sonographers Guide To The Assessment oDocument1 pageA Sonographers Guide To The Assessment orohanjee277No ratings yet
- Cardiac Arrhythmias Cardiac ArrhythmiasDocument29 pagesCardiac Arrhythmias Cardiac ArrhythmiasgowthamNo ratings yet
- Cardiology Professor Discusses ACS Diagnosis and ManagementDocument34 pagesCardiology Professor Discusses ACS Diagnosis and ManagementAyeshah IlyasNo ratings yet
- Peritoneal Dialysis Unit Renal Department SGH PD WPI 097 Workplace InstructionDocument10 pagesPeritoneal Dialysis Unit Renal Department SGH PD WPI 097 Workplace InstructionAjeng SuparwiNo ratings yet
- Apache II ScoringDocument1 pageApache II ScoringBindusagar PattanaikNo ratings yet
- Pem. Cardiovaskular Dr. MulyadiDocument195 pagesPem. Cardiovaskular Dr. MulyadiBettry Ahmad100% (1)
- Facts About Sudden Cardiac ArrestDocument2 pagesFacts About Sudden Cardiac ArrestZeljko LekovicNo ratings yet
- KDOQI Clinical Practice Guideline Hemodialysis Update - Public Review Draft FINAL - 20150204 PDFDocument78 pagesKDOQI Clinical Practice Guideline Hemodialysis Update - Public Review Draft FINAL - 20150204 PDFศักดิ์ชัย พูนศรีเจริญกุลNo ratings yet
- Diploma in Cath Lab TechnologyDocument3 pagesDiploma in Cath Lab TechnologyOmprakash NinamaNo ratings yet
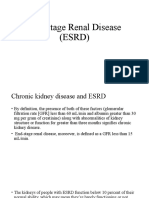
- End Stage Renal Disease (ESRD)Document21 pagesEnd Stage Renal Disease (ESRD)Dani DanyNo ratings yet
- Step by Step EchocardiographyDocument141 pagesStep by Step EchocardiographyMonica Surdu83% (6)
- Ipd - KardiologiDocument116 pagesIpd - KardiologiWynda MuljonoNo ratings yet
- NCM 118 ReviewerDocument14 pagesNCM 118 ReviewerMarceil MortelNo ratings yet
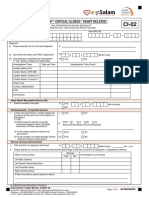
- CI 02 Heart RelatedDocument2 pagesCI 02 Heart RelatedSiti Rohani AhmadNo ratings yet
- Discussion RsovDocument30 pagesDiscussion RsovwarholeblackNo ratings yet
- Ecg Made EasyDocument45 pagesEcg Made Easyfisiopop100% (4)
- Clinical Fellow Job in General Internal MedicineDocument9 pagesClinical Fellow Job in General Internal MedicineQusaiBadrNo ratings yet
- ACLS Algorithms 2020 (Advanced Cardiac Life Support)Document1 pageACLS Algorithms 2020 (Advanced Cardiac Life Support)evelyn k100% (2)
- 118 Skills Lab-Week 2-ECG TakingDocument8 pages118 Skills Lab-Week 2-ECG TakingKeisha BartolataNo ratings yet
- Cardio QuestionsDocument18 pagesCardio QuestionsTrisha ArizalaNo ratings yet
- Angina Stable vs. UnstableDocument1 pageAngina Stable vs. UnstableAlther LorenNo ratings yet