You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The BSN Job Search: Interview Preparation: Telling Your StoryDocument25 pagesThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohNo ratings yet
- Random FactsDocument338 pagesRandom Factscyram81100% (1)
- King Rush MoreDocument1 pageKing Rush MoreawuahbohNo ratings yet
- Oop Say You Know MeDocument1 pageOop Say You Know MeawuahbohNo ratings yet
- EBP Article 3Document6 pagesEBP Article 3awuahbohNo ratings yet
- Probability of A or B and A and B-1Document2 pagesProbability of A or B and A and B-1awuahbohNo ratings yet
- HandOff SampleToolsDocument9 pagesHandOff SampleToolsOllie EvansNo ratings yet
- Article For JournalDocument6 pagesArticle For JournalawuahbohNo ratings yet
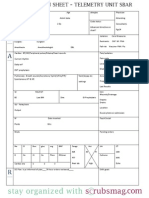
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624No ratings yet
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohNo ratings yet
- Pharm NclexDocument9 pagesPharm NclexawuahbohNo ratings yet
- Drugs NclexDocument30 pagesDrugs Nclexawuahboh100% (1)
- NCLEX Random FactsDocument34 pagesNCLEX Random FactsLegnaMary100% (8)
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Document23 pagesMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohNo ratings yet
- PolypharmacyDocument24 pagesPolypharmacySurina Zaman HuriNo ratings yet
- Massachusetts Department of Public HealthDocument24 pagesMassachusetts Department of Public HealthawuahbohNo ratings yet
- ENT Throat and EsophagusDocument41 pagesENT Throat and EsophagusMUHAMMAD HASAN NAGRANo ratings yet
- EBP Article 1Document11 pagesEBP Article 1awuahbohNo ratings yet
- Patient Report FormDocument1 pagePatient Report FormawuahbohNo ratings yet
- STDA VaricealDocument8 pagesSTDA VaricealDeisy de JesusNo ratings yet
- Critical Thinking StrategiesDocument3 pagesCritical Thinking StrategiesawuahbohNo ratings yet
- Tips On Answering NclexDocument4 pagesTips On Answering NclexawuahbohNo ratings yet
- Therapeutic CommunicationDocument1 pageTherapeutic CommunicationawuahbohNo ratings yet
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocument24 pagesDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohNo ratings yet
- Debate 3 Youth Incarceration in Adult PrisonsDocument6 pagesDebate 3 Youth Incarceration in Adult PrisonsawuahbohNo ratings yet
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohNo ratings yet
- Parkland formula and rule of 9Document8 pagesParkland formula and rule of 9awuahbohNo ratings yet
- Article For JournalDocument6 pagesArticle For JournalawuahbohNo ratings yet
- Article For Journal 4-18-14Document8 pagesArticle For Journal 4-18-14awuahbohNo ratings yet
- Article For Jouranal 2 (498P)Document5 pagesArticle For Jouranal 2 (498P)awuahbohNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- A Literature Review of Application of Sifeng Point (EX-UE 10) in Children KoreaDocument18 pagesA Literature Review of Application of Sifeng Point (EX-UE 10) in Children KoreashalyhasnyNo ratings yet
- Sherman (1998) - Evidence-Based PolicingDocument16 pagesSherman (1998) - Evidence-Based PolicingPoliceFoundationNo ratings yet
- Case Write-Up 2Document22 pagesCase Write-Up 2Syed TalhaNo ratings yet
- Volatile AnestheticsDocument16 pagesVolatile AnestheticsDhonz R AdiwaramanNo ratings yet
- 필라테스 논문Document6 pages필라테스 논문Kang Hoon KimNo ratings yet
- Early MobilizationDocument9 pagesEarly MobilizationBlake BoggenpoelNo ratings yet
- Yamada Et Al 2023 2023 American Heart Association and American Academy of Pediatrics Focused Update On NeonatalDocument10 pagesYamada Et Al 2023 2023 American Heart Association and American Academy of Pediatrics Focused Update On NeonatalKarine SchmidtNo ratings yet
- 5 Essentials For Effective Evaluation FA AADocument8 pages5 Essentials For Effective Evaluation FA AALucy RoseNo ratings yet
- Anna-Paulina Wiedel Fixed or Removable Appliance For Early Orthodontic Treatment of Functional ... (PDFDrive) PDFDocument112 pagesAnna-Paulina Wiedel Fixed or Removable Appliance For Early Orthodontic Treatment of Functional ... (PDFDrive) PDFYasmin SherifNo ratings yet
- Brain Waves InfoDocument46 pagesBrain Waves Infoedukit8606No ratings yet
- Geriatrics 04 00068 s001Document15 pagesGeriatrics 04 00068 s001Rashmi SheelvantNo ratings yet
- Handwashing For Preventing DiarrhoeaDocument44 pagesHandwashing For Preventing DiarrhoeaSTBM IndonesiaNo ratings yet
- A Critical Review of The Scientist Practitioner Model For Counselling PsychologyDocument13 pagesA Critical Review of The Scientist Practitioner Model For Counselling PsychologySanja DjordjevicNo ratings yet
- Quantitative Research PowerPointDocument3 pagesQuantitative Research PowerPointMathembe KENo ratings yet
- Glossary of Statistical TermsDocument20 pagesGlossary of Statistical TermsRobertNo ratings yet
- (CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesDocument194 pages(CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesBianca Watanabe - RatillaNo ratings yet
- Hypno 1Document7 pagesHypno 1Eka AfriliaNo ratings yet
- International Journal of Research in Pharmacy and ScienceDocument16 pagesInternational Journal of Research in Pharmacy and ScienceCdma Nastiti FatimahNo ratings yet
- Adverse Events Reported From Hyaluronic Acid Dermal Filler Injections To The Facial Region - A Systematic Review and Meta-AnalysisDocument16 pagesAdverse Events Reported From Hyaluronic Acid Dermal Filler Injections To The Facial Region - A Systematic Review and Meta-AnalysisArcelino FariasNo ratings yet
- Post Normal Futures Kritik UTNIF 2012Document236 pagesPost Normal Futures Kritik UTNIF 2012Jacob LundquistNo ratings yet
- Journal Pembanding 2 Kala 2 PersalinanDocument15 pagesJournal Pembanding 2 Kala 2 PersalinanBalqis Mumtaz YousanNo ratings yet
- Guidelines For Evaluation and Management of LBPDocument482 pagesGuidelines For Evaluation and Management of LBPShashi JainNo ratings yet
- Sainani Et Al 2011 PM&RDocument5 pagesSainani Et Al 2011 PM&RHarshil DaveNo ratings yet
- Difficult Decisions in Colorectal PDFDocument578 pagesDifficult Decisions in Colorectal PDFDenise Guevara100% (1)
- Protocol Writing in ClinicalDocument72 pagesProtocol Writing in ClinicalNashwan ANo ratings yet
- The Efficacy of Manual Therapy For Rotator Cuff Tendinopathy: A Systematic Review and Meta AnalysisDocument21 pagesThe Efficacy of Manual Therapy For Rotator Cuff Tendinopathy: A Systematic Review and Meta AnalysisJacinta SeguraNo ratings yet
- KNGF-guideline Stroke Practice Guidelines 2014 EnglishDocument73 pagesKNGF-guideline Stroke Practice Guidelines 2014 EnglishHarfika NovianaNo ratings yet
- Nutrition Therapy in Critical Illness: A Review of The Literature For CliniciansDocument11 pagesNutrition Therapy in Critical Illness: A Review of The Literature For CliniciansRamon Sureda BalcellsNo ratings yet
- The JASPER Model For Children With Autism Promoting Joint Attention, Symbolic Play, Engagement, and RegulationDocument381 pagesThe JASPER Model For Children With Autism Promoting Joint Attention, Symbolic Play, Engagement, and Regulationana villares100% (2)