You might also like
- Eng PDFDocument214 pagesEng PDFafriantoNo ratings yet
- ContraceptionDocument42 pagesContraceptionDyah Putri Ayu DinastyarNo ratings yet
- Halal Critical Point of Foods and Beverages - REV-1Document44 pagesHalal Critical Point of Foods and Beverages - REV-1Dyah Putri Ayu DinastyarNo ratings yet
- Preparation of Soap Using Different Types of Oils and Exploring Its Properties PDFDocument42 pagesPreparation of Soap Using Different Types of Oils and Exploring Its Properties PDFm.cj1No ratings yet
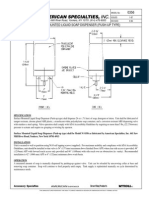
- Surface Mounted Liquid Soap Dispenser (Push-Up Type) : 441 Saw Mill River Road, Yonkers, NY 10701 (914) 476-9000Document1 pageSurface Mounted Liquid Soap Dispenser (Push-Up Type) : 441 Saw Mill River Road, Yonkers, NY 10701 (914) 476-9000Dyah Putri Ayu DinastyarNo ratings yet
- Bahaya Makanan HaramDocument37 pagesBahaya Makanan HaramDyah Putri Ayu DinastyarNo ratings yet
- Coagulation DisorderDocument36 pagesCoagulation DisorderDyah Putri Ayu DinastyarNo ratings yet
- Archive of SID: Riginal RticleDocument4 pagesArchive of SID: Riginal RticleDyah Putri Ayu DinastyarNo ratings yet
- Cocamide DEADocument1 pageCocamide DEADyah Putri Ayu DinastyarNo ratings yet
- Formulation and evaluation of herbal anti-dandruff shampooDocument5 pagesFormulation and evaluation of herbal anti-dandruff shampoofaizawidiNo ratings yet
- Ashtiani Vol18Document18 pagesAshtiani Vol18Dyah Putri Ayu DinastyarNo ratings yet
- Sodium Lauryl SulfateDocument9 pagesSodium Lauryl SulfateMoxzJr VianzNo ratings yet
- The Malassezia Genus in Skin and Systemic DiseasesDocument36 pagesThe Malassezia Genus in Skin and Systemic DiseasesDyah Putri Ayu DinastyarNo ratings yet
- Green Tea (Camellia Sinensis, L.) Ethanolic Extract As Hair Tonic in Nutraceutical: Physical Stability, Hair Growth Activity On Rats, and Safety TestDocument6 pagesGreen Tea (Camellia Sinensis, L.) Ethanolic Extract As Hair Tonic in Nutraceutical: Physical Stability, Hair Growth Activity On Rats, and Safety TestDyah Putri Ayu DinastyarNo ratings yet
- The Treatment of Dandruff of The Scalp: Harmacology CosmetologDocument8 pagesThe Treatment of Dandruff of The Scalp: Harmacology CosmetologDyah Putri Ayu DinastyarNo ratings yet
- Katakana Chart - カタカナ PDFDocument1 pageKatakana Chart - カタカナ PDFDoni SetiawanNo ratings yet
- 3162 3646 1 SMDocument7 pages3162 3646 1 SMjlekzzzNo ratings yet
- How To Make Hair ShampoosDocument1 pageHow To Make Hair Shampoospakde jongkoNo ratings yet
- Formulation and evaluation of herbal anti-dandruff shampooDocument5 pagesFormulation and evaluation of herbal anti-dandruff shampoofaizawidiNo ratings yet
- 559 PDFDocument4 pages559 PDFDyah Putri Ayu DinastyarNo ratings yet
- 106 GuptaDocument5 pages106 GuptaDyah Putri Ayu DinastyarNo ratings yet
- Jocpr 26Document7 pagesJocpr 26sumendersinghNo ratings yet
- Sen PR 0011Document12 pagesSen PR 0011Dyah Putri Ayu DinastyarNo ratings yet
- Micro Manual EngDocument262 pagesMicro Manual EngEmad ManniNo ratings yet
- Hiragana Chart - ひらがな PDFDocument1 pageHiragana Chart - ひらがな PDFDoni SetiawanNo ratings yet
- r600 Part 1Document36 pagesr600 Part 1Dyah Putri Ayu DinastyarNo ratings yet
- Sinesis L.) Dalam Sediaan Krim Terhadap Sifat Fisik Dan AktivitasDocument10 pagesSinesis L.) Dalam Sediaan Krim Terhadap Sifat Fisik Dan AktivitasDyah Putri Ayu DinastyarNo ratings yet
- Screening For The Antimicrobial Activities of Alcoholic and Aqueous Extracts of Some Common Spices in EgyptDocument8 pagesScreening For The Antimicrobial Activities of Alcoholic and Aqueous Extracts of Some Common Spices in EgyptDyah Putri Ayu DinastyarNo ratings yet
- Ijapsbs 2.3 149-155Document7 pagesIjapsbs 2.3 149-155Dyah Putri Ayu DinastyarNo ratings yet
- Formulation and Evaluation of Herbal Shampoo From: ISSN 2229-3566 Research ArticleDocument5 pagesFormulation and Evaluation of Herbal Shampoo From: ISSN 2229-3566 Research ArticleJorge Sergio CondeNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Data 25-01-2021 Jadwal Ujian CBT Umum Sektor Manufaktur Tahun 2020 Gelombang 2 SemarangDocument189 pagesData 25-01-2021 Jadwal Ujian CBT Umum Sektor Manufaktur Tahun 2020 Gelombang 2 SemarangArdhi Imron SholihinNo ratings yet
- 0610 w19 QP 41 PDFDocument20 pages0610 w19 QP 41 PDFrachitNo ratings yet
- Arachnoid Granulations PDFDocument5 pagesArachnoid Granulations PDFsebacosNo ratings yet
- Esophageal Cancer NewDocument52 pagesEsophageal Cancer Newapi-282115150No ratings yet
- Treating A Bartholins Cyst or Abscess Patient InformationDocument6 pagesTreating A Bartholins Cyst or Abscess Patient InformationRezaFArthaNo ratings yet
- Collaborative Drug Therapy ManagementDocument10 pagesCollaborative Drug Therapy ManagementAyu Dina UnifahNo ratings yet
- Real People, Real Stories: "Normally We Do Not So Much Look at Things As Overlook Them." - Alan WattsDocument18 pagesReal People, Real Stories: "Normally We Do Not So Much Look at Things As Overlook Them." - Alan WattssivanNo ratings yet
- EE MOCK Test 2 Jan 2017 Questions OnlyDocument28 pagesEE MOCK Test 2 Jan 2017 Questions OnlyEmadSamirNo ratings yet
- Module Essential Newborn CareDocument26 pagesModule Essential Newborn CareMichtropolisNo ratings yet
- Sementara Revisi Manuskrip GitaDocument13 pagesSementara Revisi Manuskrip GitaIndah Gita CahyaniNo ratings yet
- Rendam Kaki Air Hangat Insomnia PDFDocument7 pagesRendam Kaki Air Hangat Insomnia PDFNdar Screen ShootNo ratings yet
- 1 s2.0 S0269749120365866 MainDocument10 pages1 s2.0 S0269749120365866 MainPEDRO NETO DOMINGOS SIGUIMNo ratings yet
- Antihuman Globulin TestsDocument6 pagesAntihuman Globulin TestsElla OrtegaNo ratings yet
- Bipolar Disorder Treatment: Psychosocial Therapies Augment Medication to Improve Outcomes and Reduce DisabilityDocument26 pagesBipolar Disorder Treatment: Psychosocial Therapies Augment Medication to Improve Outcomes and Reduce DisabilityChristine EnriquezNo ratings yet
- Pahnke, W.N. Et Al. (1970) The Experiemental Use of Psychedelic (LSD) PsychotherapyDocument8 pagesPahnke, W.N. Et Al. (1970) The Experiemental Use of Psychedelic (LSD) PsychotherapyJeangenNo ratings yet
- Unfinished RRL Autosaved AutosavedDocument11 pagesUnfinished RRL Autosaved AutosavedNiño Bryle M. LimotanNo ratings yet
- Army Life - Your Guide To The Medical ServicesDocument15 pagesArmy Life - Your Guide To The Medical Servicesdemarchi2330No ratings yet
- BioPsych Lecture Notes CH 7Document6 pagesBioPsych Lecture Notes CH 7Generic_Persona100% (1)
- Ruskin BondDocument75 pagesRuskin BondNikchen TamangNo ratings yet
- JIPMER 2000: Ans. B 2. Which of The Following Is Not A Content of The Pudendal CanalDocument48 pagesJIPMER 2000: Ans. B 2. Which of The Following Is Not A Content of The Pudendal CanalLakshmidevi.R.M R.MNo ratings yet
- Antibacterial Activity of Garlic Extract Against E. ColiDocument24 pagesAntibacterial Activity of Garlic Extract Against E. Colinicole47920% (5)
- Nutritional Values and Pharmacological Importance of Date Fruit (Phoenix Dactylifera Linn) A ReviewDocument4 pagesNutritional Values and Pharmacological Importance of Date Fruit (Phoenix Dactylifera Linn) A ReviewDr. Md. Shahab UddinNo ratings yet
- NDocument136 pagesNLove HumanNo ratings yet
- Effect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialDocument8 pagesEffect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialH Yudi IriantoNo ratings yet
- The Anatomy and Regulation of Cerebral Blood FlowDocument33 pagesThe Anatomy and Regulation of Cerebral Blood FlowKadek Dwipa DyatmikaNo ratings yet
- Magic Roadshow 6Document87 pagesMagic Roadshow 6RickNo ratings yet
- Deviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument13 pagesDeviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Bioinformatics PaperDocument8 pagesBioinformatics PaperrashigaurNo ratings yet
- Societe Belge de Biochimie Et de Biologie Moleculaire Belgische Vereniging Voor Biochemie en Moleculaire BiologieDocument30 pagesSociete Belge de Biochimie Et de Biologie Moleculaire Belgische Vereniging Voor Biochemie en Moleculaire BiologieAmirNo ratings yet
- IEN 420: Environmental & Safety Engineering Spring 2021-2022Document34 pagesIEN 420: Environmental & Safety Engineering Spring 2021-2022Moh HNo ratings yet