You might also like
- The politics of health promotion: Case studies from Denmark and EnglandFrom EverandThe politics of health promotion: Case studies from Denmark and EnglandNo ratings yet
- Public Health Future EngDocument19 pagesPublic Health Future EngKiros Tilahun BentiNo ratings yet
- New Health Systems: Integrated Care and Health Inequalities ReductionFrom EverandNew Health Systems: Integrated Care and Health Inequalities ReductionNo ratings yet
- The Mixed Health Systems Syndrome: Sania NishtarDocument2 pagesThe Mixed Health Systems Syndrome: Sania Nishtarapi-112905159No ratings yet
- Health Care SystemsDocument10 pagesHealth Care SystemsThembaNo ratings yet
- Primary Health Care WHO OverviewDocument16 pagesPrimary Health Care WHO OverviewlilaningNo ratings yet
- Sanitation Problem Health SectorDocument44 pagesSanitation Problem Health SectordeliapatrisaNo ratings yet
- Building Resilient Communities for HealthDocument18 pagesBuilding Resilient Communities for HealthWIlfred bengnwiNo ratings yet
- Health Law AssignmentDocument2 pagesHealth Law AssignmentShubh Dixit0% (1)
- The Private Sector,: Universal Health Coverage and Primary Health CareDocument12 pagesThe Private Sector,: Universal Health Coverage and Primary Health CareJohn Aries CabilingNo ratings yet
- 7c0a PDFDocument17 pages7c0a PDFAngelica RojasNo ratings yet
- Sociology GovernmentDocument6 pagesSociology Governmentgloriabala92No ratings yet
- Primary Health Care 2007 enDocument42 pagesPrimary Health Care 2007 enAC GanadoNo ratings yet
- Ibrahim Halliru T-PDocument23 pagesIbrahim Halliru T-PUsman Ahmad TijjaniNo ratings yet
- Community Nursing and Care Continuity LEARNING OUTCOMES After CompletingDocument23 pagesCommunity Nursing and Care Continuity LEARNING OUTCOMES After Completingtwy113100% (1)
- Government's Policy on Public HealthDocument30 pagesGovernment's Policy on Public HealthKrittika PatelNo ratings yet
- Public Health CourseworkDocument12 pagesPublic Health CourseworkAndrew AkamperezaNo ratings yet
- Jakarta Declaration On Leading Health Promotion Into The 21st CenturyDocument4 pagesJakarta Declaration On Leading Health Promotion Into The 21st CenturyWayne Ivan DugayNo ratings yet
- Chapter 7Document9 pagesChapter 7Lawrence Ryan DaugNo ratings yet
- Ijerph 17 04363 v3Document26 pagesIjerph 17 04363 v3biruckNo ratings yet
- Un Platform FinalDocument18 pagesUn Platform FinalAginaya ReinNo ratings yet
- Globalisation and Health: Challenges: Go ToDocument3 pagesGlobalisation and Health: Challenges: Go ToRembrant FernandezNo ratings yet
- Public Health-Its RegulationDocument12 pagesPublic Health-Its RegulationAreeb AhmadNo ratings yet
- KemerutDocument2 pagesKemerutFrance Nathaniel CanaleNo ratings yet
- Building The Primary of The 21st Century: Health Care WorkforceDocument32 pagesBuilding The Primary of The 21st Century: Health Care Workforcelucila falconeNo ratings yet
- National & Sttae Health Care Policy, National Population Policy, AyushDocument52 pagesNational & Sttae Health Care Policy, National Population Policy, Ayushkrishnasree100% (2)
- How Can HealthDocument43 pagesHow Can HealthMaria TricasNo ratings yet
- Recife Declaration 13nov PDFDocument4 pagesRecife Declaration 13nov PDFSá LealNo ratings yet
- SummaryDocument1 pageSummaryVasquez MicoNo ratings yet
- Primary Health Care Approach Outlined in Alma Ata DeclarationDocument5 pagesPrimary Health Care Approach Outlined in Alma Ata DeclarationFlorenze Laiza Donor Lucas100% (1)
- Framework On Integrated People-Centred Health Services (IPCHS)Document23 pagesFramework On Integrated People-Centred Health Services (IPCHS)Merty ReferendumNo ratings yet
- 1 JOOUST FUNDAMENTALS HOME ASSIGNMENTDocument9 pages1 JOOUST FUNDAMENTALS HOME ASSIGNMENTosundwahronnieNo ratings yet
- Savedoff de Ferranti & Smith Et Al 2012 Aspects of Transition To UHCDocument9 pagesSavedoff de Ferranti & Smith Et Al 2012 Aspects of Transition To UHCashakow8849No ratings yet
- National Health Policies 2 ND YearDocument40 pagesNational Health Policies 2 ND YearLIDIYA MOL P VNo ratings yet
- 5 StarDocument13 pages5 StarSofie Hanafiah NuruddhuhaNo ratings yet
- Health needs assessment: Understanding community health prioritiesDocument47 pagesHealth needs assessment: Understanding community health prioritieshanoo777No ratings yet
- Health Care Guide Provides Overview of Systems and ForecastsDocument203 pagesHealth Care Guide Provides Overview of Systems and ForecastsNiro ThakurNo ratings yet
- Hospital AdministrationDocument41 pagesHospital AdministrationAnkita VishwakarmaNo ratings yet
- Towards An Equitable People-Centred Health System For SpainDocument3 pagesTowards An Equitable People-Centred Health System For SpainrevistesperllegirNo ratings yet
- UHC Country Support PDFDocument12 pagesUHC Country Support PDFdiah irfainiNo ratings yet
- Community-Based Health Insurance in Developing CountriesDocument14 pagesCommunity-Based Health Insurance in Developing CountriesRakip MaloskiNo ratings yet
- The Public Private Partnership Has Been Defined by Different Organization As FollowsDocument3 pagesThe Public Private Partnership Has Been Defined by Different Organization As FollowsViru JaniNo ratings yet
- Achieving Better Health for All Through Primary Health CareDocument6 pagesAchieving Better Health for All Through Primary Health CareRem Alfelor100% (1)
- Primary Health Care I 2021Document13 pagesPrimary Health Care I 2021Galakpai KolubahNo ratings yet
- Review of Social Determinants and The Health Divide in The WHO European RegionDocument234 pagesReview of Social Determinants and The Health Divide in The WHO European RegionAdrian ArizmendiNo ratings yet
- Salud 2020Document14 pagesSalud 2020Jorge Mandl StanglNo ratings yet
- Framework On Integrated People Centred Health ServicesDocument12 pagesFramework On Integrated People Centred Health Servicesaperfectcircle7978No ratings yet
- Intersectoral coordination improves health careDocument26 pagesIntersectoral coordination improves health carelimiya vargheseNo ratings yet
- Health Policy of Ethiopia 1993Document11 pagesHealth Policy of Ethiopia 1993Hayleye KinfeNo ratings yet
- Intersectoral Coordination in India For Health Care AdvancementDocument26 pagesIntersectoral Coordination in India For Health Care AdvancementshijoantonyNo ratings yet
- 2.07-4.6 Global Fund Strategic Approach To HSS. WHO ReportDocument50 pages2.07-4.6 Global Fund Strategic Approach To HSS. WHO ReportGeorge KorahNo ratings yet
- HSRA: Fourmula One for Health Reform AgendaDocument3 pagesHSRA: Fourmula One for Health Reform AgendaMadsNo ratings yet
- AhaDocument6 pagesAhaFlorito Jc EspirituNo ratings yet
- The Health Care Delivery SystemDocument34 pagesThe Health Care Delivery SystemFritzie Buquiron67% (3)
- World Health Organization: Discussion PaperDocument65 pagesWorld Health Organization: Discussion PaperJimNo ratings yet
- Assignment: Primary Health Care and Its Components in Detail in The Light of Almata DeclarationDocument11 pagesAssignment: Primary Health Care and Its Components in Detail in The Light of Almata DeclarationfurqanazeemiNo ratings yet
- Unit 8 Task 1Document10 pagesUnit 8 Task 1dk5kbmqg7sNo ratings yet
- The Lancet - Vol. 0376 - 2010.11.27Document79 pagesThe Lancet - Vol. 0376 - 2010.11.27Patty HabibiNo ratings yet
- Un Marco de Resultados de Salud PublicaDocument52 pagesUn Marco de Resultados de Salud PublicaJorge Mandl StanglNo ratings yet
- Icd 10 Code Klinik DR KeluargaDocument6 pagesIcd 10 Code Klinik DR Keluargaferry7765No ratings yet
- Fitness Travel Assessment FormDocument1 pageFitness Travel Assessment Formferry7765No ratings yet
- Modern View On The ChannelsDocument6 pagesModern View On The Channelsferry7765No ratings yet
- Acupuncture ObesityDocument4 pagesAcupuncture Obesityferry7765100% (1)
- Khusha NofashaDocument1 pageKhusha Nofashaferry7765No ratings yet
- Base Line Health Assessment For PrintedDocument3 pagesBase Line Health Assessment For Printedferry7765No ratings yet
- MERS CoV Investigation Guideline Jul13Document40 pagesMERS CoV Investigation Guideline Jul13ferry7765No ratings yet
- Icd 10Document1 pageIcd 10ferry7765No ratings yet
- Acupuncture Case SeriesDocument8 pagesAcupuncture Case Seriesferry7765No ratings yet
- Base Line Health Assessment For PrintedDocument3 pagesBase Line Health Assessment For Printedferry7765No ratings yet
- Daily Report of Doctor ConsultationDocument1 pageDaily Report of Doctor Consultationferry7765No ratings yet
- Care for patients of all ages and communitiesDocument2 pagesCare for patients of all ages and communitiesferry7765No ratings yet
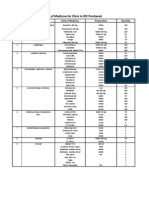
- List of Medicines For Pontianak April 2014Document2 pagesList of Medicines For Pontianak April 2014ferry7765No ratings yet
- SOAP Form For Daily Medical ConsultationDocument2 pagesSOAP Form For Daily Medical Consultationferry7765No ratings yet
- SOAP Form For Daily Medical ConsultationDocument2 pagesSOAP Form For Daily Medical Consultationferry7765No ratings yet
- Patients Registration ListDocument2 pagesPatients Registration Listferry7765No ratings yet
- Koriko LomDocument1 pageKoriko Lomferry7765No ratings yet
- Win. Loader W7Document26 pagesWin. Loader W7Roberto Giner PérezNo ratings yet
- Diabetes Flow SheetDocument2 pagesDiabetes Flow Sheetferry7765No ratings yet
- Contraction of The Five Fingers LU-6, L.I.-3, L.I.-5, SI-4, SJ-2, SJ-3, LIV-3 Lu 5 Si 7Document1 pageContraction of The Five Fingers LU-6, L.I.-3, L.I.-5, SI-4, SJ-2, SJ-3, LIV-3 Lu 5 Si 7ferry7765No ratings yet
- List of Medicines For Pontianak April 2014Document2 pagesList of Medicines For Pontianak April 2014ferry7765No ratings yet
- Young Ti Ying Quan XiDocument6 pagesYoung Ti Ying Quan Xiferry7765No ratings yet
- Stroke LengkapDocument3 pagesStroke Lengkapferry7765No ratings yet
- Daftar Judul Buku Yang Saya PunyaDocument1 pageDaftar Judul Buku Yang Saya Punyaferry7765No ratings yet
- Contraction of The Five Fingers LU-6, L.I.-3, L.I.-5, SI-4, SJ-2, SJ-3, LIV-3 Lu 5 Si 7Document1 pageContraction of The Five Fingers LU-6, L.I.-3, L.I.-5, SI-4, SJ-2, SJ-3, LIV-3 Lu 5 Si 7ferry7765No ratings yet
- Participant ID Date Received 1st Keying Assigned To 2nd Keying Assigned To Problems Solutions NotesDocument1 pageParticipant ID Date Received 1st Keying Assigned To 2nd Keying Assigned To Problems Solutions Notesferry7765No ratings yet
- Alamat P CareDocument1 pageAlamat P Careferry7765No ratings yet
- Time Sheet 21 April 2014 To 20 May 2014Document1 pageTime Sheet 21 April 2014 To 20 May 2014ferry7765No ratings yet
- Khusha NofashaDocument1 pageKhusha Nofashaferry7765No ratings yet
- Jurnal DMDocument13 pagesJurnal DMidaNo ratings yet
- Golden Berry Bioautography Reveals Antibacterial CompoundsDocument11 pagesGolden Berry Bioautography Reveals Antibacterial CompoundsGeraldineMoletaGabutinNo ratings yet
- Third Quarter Summative Test No. 4 EnglishDocument3 pagesThird Quarter Summative Test No. 4 EnglishJoanaNo ratings yet
- Coronavirus British English Intermediate b1 b2 GroupDocument4 pagesCoronavirus British English Intermediate b1 b2 GroupAngel AnitaNo ratings yet
- Studies in History and Philosophy of Science: Eliminative Abduction in MedicineDocument8 pagesStudies in History and Philosophy of Science: Eliminative Abduction in MedicineFede FestaNo ratings yet
- Canine Disobedient, Unruly and ExcitableDocument5 pagesCanine Disobedient, Unruly and ExcitableBrook Farm Veterinary CenterNo ratings yet
- Terminologia LatinaDocument7 pagesTerminologia LatinaКонстантин ЗахарияNo ratings yet
- VSL TB Workplace Policy ProgramDocument3 pagesVSL TB Workplace Policy ProgramAlexander John AlixNo ratings yet
- Marking Scheme: Biology Paper 3Document4 pagesMarking Scheme: Biology Paper 3sybejoboNo ratings yet
- Pharmacology - Tot - NR 6classid S.F.ADocument74 pagesPharmacology - Tot - NR 6classid S.F.AcorsairmdNo ratings yet
- Word Parts Dictionary, Prefixes, Suffixes, Roots and Combining FormsDocument237 pagesWord Parts Dictionary, Prefixes, Suffixes, Roots and Combining Formslaukings100% (9)
- Ananda Zaren - Core Elements of The Materia Medica of The Mind - Vol IDocument101 pagesAnanda Zaren - Core Elements of The Materia Medica of The Mind - Vol Ialex100% (2)
- Organ Transplantatio1Document26 pagesOrgan Transplantatio1Bindashboy0No ratings yet
- EXP 6 - Fecal Coliform Test - StudentDocument8 pagesEXP 6 - Fecal Coliform Test - StudentAbo SmraNo ratings yet
- How Can Women Make The RulesDocument0 pagesHow Can Women Make The Ruleshme_s100% (2)
- Homeoapthy For InfantsDocument9 pagesHomeoapthy For Infantspavani_upNo ratings yet
- ShaylaDocument3 pagesShaylaapi-530728661No ratings yet
- M1 ReadingwritingDocument8 pagesM1 ReadingwritingChing ServandoNo ratings yet
- PMO - Pasteurized Milk OrdinanceDocument340 pagesPMO - Pasteurized Milk OrdinanceTato G.k.No ratings yet
- Dangers of Excess Sugar ConsumptionDocument2 pagesDangers of Excess Sugar ConsumptionAIDEN COLLUMSDEANNo ratings yet
- 13 Levels of AssessmentDocument11 pages13 Levels of AssessmentCatherine Cayda dela Cruz-BenjaminNo ratings yet
- 10 DOH Approved Herbal Medicine: Prepared By: Washington, Luis D. Student Nurse BSN 2H-DDocument11 pages10 DOH Approved Herbal Medicine: Prepared By: Washington, Luis D. Student Nurse BSN 2H-DLuis WashingtonNo ratings yet
- Soal BAHASA INGGRIS - X - KUMER - PAKET 2Document13 pagesSoal BAHASA INGGRIS - X - KUMER - PAKET 2Agus SuhendraNo ratings yet
- Nat Ag Winter Wheat in N Europe by Marc BonfilsDocument5 pagesNat Ag Winter Wheat in N Europe by Marc BonfilsOrto di CartaNo ratings yet
- AIPG Paper CorrectedDocument42 pagesAIPG Paper CorrectedbrihaspathiacademyNo ratings yet
- Types of Feeding TubesDocument8 pagesTypes of Feeding TubesElda KuizonNo ratings yet
- A Novel Lymphocyte Transformation Test (LTT-MELISAR) For Lyme BorreliosisDocument8 pagesA Novel Lymphocyte Transformation Test (LTT-MELISAR) For Lyme Borreliosisdebnathsuman49No ratings yet
- The Impact of Life Cycles on Family HealthDocument27 pagesThe Impact of Life Cycles on Family Healthmarcial_745578124No ratings yet
- Diane Pills Drug StudyDocument4 pagesDiane Pills Drug StudyDawn EncarnacionNo ratings yet
- Detailed Project Report (DPR) :model Template: For NHB Scheme No.1 For AonlaDocument136 pagesDetailed Project Report (DPR) :model Template: For NHB Scheme No.1 For AonlajainendraNo ratings yet
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherFrom EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNo ratings yet
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4.5 out of 5 stars4.5/5 (32)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 5 out of 5 stars5/5 (36)
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4 out of 5 stars4/5 (19)
- Poor Economics: A Radical Rethinking of the Way to Fight Global PovertyFrom EverandPoor Economics: A Radical Rethinking of the Way to Fight Global PovertyRating: 4.5 out of 5 stars4.5/5 (263)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- High-Risers: Cabrini-Green and the Fate of American Public HousingFrom EverandHigh-Risers: Cabrini-Green and the Fate of American Public HousingNo ratings yet
- Hillbilly Elegy: A Memoir of a Family and Culture in CrisisFrom EverandHillbilly Elegy: A Memoir of a Family and Culture in CrisisRating: 4 out of 5 stars4/5 (4276)
- Fucked at Birth: Recalibrating the American Dream for the 2020sFrom EverandFucked at Birth: Recalibrating the American Dream for the 2020sRating: 4 out of 5 stars4/5 (172)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (5)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (269)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 4 out of 5 stars4/5 (186)
- Not a Crime to Be Poor: The Criminalization of Poverty in AmericaFrom EverandNot a Crime to Be Poor: The Criminalization of Poverty in AmericaRating: 4.5 out of 5 stars4.5/5 (37)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 4 out of 5 stars4/5 (126)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (188)
- Sons, Daughters, and Sidewalk Psychotics: Mental Illness and Homelessness in Los AngelesFrom EverandSons, Daughters, and Sidewalk Psychotics: Mental Illness and Homelessness in Los AngelesNo ratings yet
- Charity Detox: What Charity Would Look Like If We Cared About ResultsFrom EverandCharity Detox: What Charity Would Look Like If We Cared About ResultsRating: 4 out of 5 stars4/5 (9)
- Alienated America: Why Some Places Thrive While Others CollapseFrom EverandAlienated America: Why Some Places Thrive While Others CollapseRating: 4 out of 5 stars4/5 (35)