You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- GIS Data Management Mapping Potential Limiting Factors To Marten Recolonization in NHDocument11 pagesGIS Data Management Mapping Potential Limiting Factors To Marten Recolonization in NHA. D. PrasadNo ratings yet
- Hasso Plattner D.school. These Are Among The 229 Students From 62 Higher Education Institutions in 10 CountriesDocument1 pageHasso Plattner D.school. These Are Among The 229 Students From 62 Higher Education Institutions in 10 CountriesA. D. PrasadNo ratings yet
- 1395Document2 pages1395A. D. PrasadNo ratings yet
- Invitation For Submission of Research Proposals: Government of India Department of Science and Technology NRDMS DivisionDocument2 pagesInvitation For Submission of Research Proposals: Government of India Department of Science and Technology NRDMS DivisionA. D. PrasadNo ratings yet
- 1396Document10 pages1396A. D. PrasadNo ratings yet
- Employees On Deputation As On 09.04.2015: S.No Name Designa Tion Date of Birth Deputated OrganizationDocument2 pagesEmployees On Deputation As On 09.04.2015: S.No Name Designa Tion Date of Birth Deputated OrganizationA. D. PrasadNo ratings yet
- Department of Civil EngineeringDocument1 pageDepartment of Civil EngineeringA. D. PrasadNo ratings yet
- National Institute of Technology Karnataka, Surathkal, Mangalore, 575 025Document1 pageNational Institute of Technology Karnataka, Surathkal, Mangalore, 575 025A. D. PrasadNo ratings yet
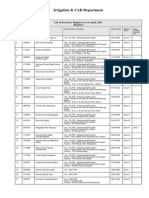
- Irrigation & CAD DepartmentDocument2 pagesIrrigation & CAD DepartmentA. D. PrasadNo ratings yet
- Faculty Contract 2015Document3 pagesFaculty Contract 2015A. D. PrasadNo ratings yet
- Archive of Sid: Assessing The Accuracy of Dems Derived From Contour Line Maps and Comparing With Aster DemsDocument3 pagesArchive of Sid: Assessing The Accuracy of Dems Derived From Contour Line Maps and Comparing With Aster DemsA. D. PrasadNo ratings yet
- KJ Hannover Workshop2013Document6 pagesKJ Hannover Workshop2013A. D. PrasadNo ratings yet
- Aster Qa Plan v2.0Document41 pagesAster Qa Plan v2.0Italo MelgarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Zeolite The Miracle (Paperback)Document58 pagesZeolite The Miracle (Paperback)Airton GuardiniNo ratings yet
- Case Study: Heavy Metals in SoilDocument4 pagesCase Study: Heavy Metals in SoilShahirah AmiraNo ratings yet
- FAQ For OSRDocument26 pagesFAQ For OSRsisi marxNo ratings yet
- Status of Sponge Iron Plant in OrissaDocument36 pagesStatus of Sponge Iron Plant in OrissachiranjibdcNo ratings yet
- Tesis Master-Ingles - 1Document8 pagesTesis Master-Ingles - 1STEFANY SHUGEY QUISPE TERANNo ratings yet
- Detoxamin Anti Aging AbstractDocument21 pagesDetoxamin Anti Aging AbstractLailatulMunawarohNo ratings yet
- SASO Standards - Plastic BottlesDocument6 pagesSASO Standards - Plastic BottlesIrfan chaudharyNo ratings yet
- Arnold Ehret - Mucusless Diet Healing System EBOKDocument2 pagesArnold Ehret - Mucusless Diet Healing System EBOKAriol ZereNo ratings yet
- Effects of Magnetically Treated Water On Germination and Growth of Tomato (Lycopersicon Esculentum: Under Poor Soil Fertility and Deficit IrrigationDocument9 pagesEffects of Magnetically Treated Water On Germination and Growth of Tomato (Lycopersicon Esculentum: Under Poor Soil Fertility and Deficit IrrigationSundeeNo ratings yet
- Monsalve Et Al. 2021. Charecterizing Potential Substrate Materials Soiless Culture SystemsDocument22 pagesMonsalve Et Al. 2021. Charecterizing Potential Substrate Materials Soiless Culture SystemsoimonsalvecNo ratings yet
- Magnetic Susceptibility and Heavy Metal Content of Palm Oil Plantations Soil As A Function of Its DepthDocument5 pagesMagnetic Susceptibility and Heavy Metal Content of Palm Oil Plantations Soil As A Function of Its DepthMittaNo ratings yet
- ASEAN GAP - Food Safety ModuleDocument69 pagesASEAN GAP - Food Safety ModuleASEAN100% (1)
- Observation of Eavy Etal Azard On Rocess Rozen Scolar IlletsDocument9 pagesObservation of Eavy Etal Azard On Rocess Rozen Scolar IlletsMuhammad Rifqi SuryantoNo ratings yet
- Limit Tests (Autosaved)Document53 pagesLimit Tests (Autosaved)Adithi ukNo ratings yet
- Debenhams Risk Assessment Matrix For Chemical Testing. V4Document6 pagesDebenhams Risk Assessment Matrix For Chemical Testing. V4Ashok Lakshmanan100% (1)
- IDT - 8 v1 Waste ManagementDocument13 pagesIDT - 8 v1 Waste ManagementOzzyNo ratings yet
- Investigation of Heavy Metal Contents in Cow Milk SamplesDocument4 pagesInvestigation of Heavy Metal Contents in Cow Milk SamplesRasha M. Almostfa JameNo ratings yet
- Cyanide Remediation: Current and Past TechnologiesDocument26 pagesCyanide Remediation: Current and Past TechnologiesCoraKiriNo ratings yet
- Guidelines On The Procedures and Technical Requirements For The Issuance of A Certification Allowing The Safe Re-Use of Wastewater For Purposes of Irrigation and Other Agricultural UsesDocument28 pagesGuidelines On The Procedures and Technical Requirements For The Issuance of A Certification Allowing The Safe Re-Use of Wastewater For Purposes of Irrigation and Other Agricultural Usesgabinuang2No ratings yet
- Dorcas ProjectDocument70 pagesDorcas ProjectJames FieworNo ratings yet
- Cilantro MilletDocument2 pagesCilantro MilletdionysiaNo ratings yet
- Frater Albertus - ParachemyDocument319 pagesFrater Albertus - Parachemytravellerfellow100% (2)
- Investigatory Project Biology LabDocument11 pagesInvestigatory Project Biology LabNorries Jonell CaballarNo ratings yet
- Hangzhou Epsilon Chemical Co.,Ltd.: Material Safety Data Sheet (MSDS)Document2 pagesHangzhou Epsilon Chemical Co.,Ltd.: Material Safety Data Sheet (MSDS)GİZEM DEMİRNo ratings yet
- Sabiu WadaDocument40 pagesSabiu WadaHamza ummusalma AliNo ratings yet
- PROJECT REPORT FinalDocument53 pagesPROJECT REPORT FinalSagarNo ratings yet
- 44-74169APP ICPOESToyAnalysisHeavyMetalDocument6 pages44-74169APP ICPOESToyAnalysisHeavyMetalMarimany Al ZarouniNo ratings yet
- Chemtrails Learn How To Protect Yourself From These Treacherous PoisonsDocument2 pagesChemtrails Learn How To Protect Yourself From These Treacherous PoisonsDarkcastle2012No ratings yet
- Journal of Indian Water Works Association (JIWWA, Vol-4, Issue-47) - Oct-Dec-2015Document80 pagesJournal of Indian Water Works Association (JIWWA, Vol-4, Issue-47) - Oct-Dec-2015Santosh Kumar100% (1)
- Introduction To Environmental Hydrogeochemistry PDFDocument106 pagesIntroduction To Environmental Hydrogeochemistry PDFJuan-CarlosPeroniZamudioNo ratings yet