You might also like
- Acog Practice Bulletin TiroidesDocument10 pagesAcog Practice Bulletin TiroidesMerpi Alvarez Goris100% (1)
- Practic Bulletin Tiroides - ACOG - OG - 2015Document10 pagesPractic Bulletin Tiroides - ACOG - OG - 2015Rich GmzNo ratings yet
- TiroidopatiasDocument10 pagesTiroidopatiasArantza PelaezNo ratings yet
- 148 Thyroid Disease in PregnancyDocument10 pages148 Thyroid Disease in Pregnancyobgin uiNo ratings yet
- Enfermedad Tiroides y Embarazo ACOGDocument10 pagesEnfermedad Tiroides y Embarazo ACOGDairo PintoNo ratings yet
- Hyperthyroidism PregnancyDocument3 pagesHyperthyroidism PregnancySyahfiq IsmailNo ratings yet
- Grave DiseaseDocument6 pagesGrave DiseaseFakrocev Charlie GuloNo ratings yet
- Cme Reviewarticle: Diagnosis and Management of Hyperthyroidism in Pregnancy: A ReviewDocument11 pagesCme Reviewarticle: Diagnosis and Management of Hyperthyroidism in Pregnancy: A ReviewErnestNo ratings yet
- Emergencias EndocrinasDocument6 pagesEmergencias EndocrinasAlex Andrés Cuevas UrriolaNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument7 pagesJournal of Clinical & Translational EndocrinologyCindyTariganNo ratings yet
- Hypertiroid PD KehamilanDocument7 pagesHypertiroid PD KehamilanAD MonikaNo ratings yet
- Bioscientific Review (BSR)Document10 pagesBioscientific Review (BSR)UMT JournalsNo ratings yet
- Enfermedades Tiroideas en El EmbarazoDocument14 pagesEnfermedades Tiroideas en El EmbarazoMelissa Gómez CruzNo ratings yet
- Thyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesDocument8 pagesThyroid Storm May Be The Initial Presentation Of: Thyrotoxicosis in Undiagnosed Children, Particularly in NeonatesLolla MorsiNo ratings yet
- Screenshot 2022-10-07 at 5.51.47 AMDocument14 pagesScreenshot 2022-10-07 at 5.51.47 AMManuel PuertaNo ratings yet
- Thyroid Storm Induced by Trauma: A Challenging CombinationDocument7 pagesThyroid Storm Induced by Trauma: A Challenging CombinationKarl Angelo MontanoNo ratings yet
- Tiroid Disease 14 HalamanDocument14 pagesTiroid Disease 14 HalamanDevi SuryandariNo ratings yet
- Hypothyroidism: Special Types of HypothyroidismDocument4 pagesHypothyroidism: Special Types of HypothyroidismVictor VicencioNo ratings yet
- Etiology-Hypothyroidism: Chronic Autoimmune ThyroiditisDocument4 pagesEtiology-Hypothyroidism: Chronic Autoimmune ThyroiditisNungky KusumaNo ratings yet
- Thyroid Disease in Pregnancy v3.6Document9 pagesThyroid Disease in Pregnancy v3.6nino.matasNo ratings yet
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocument13 pagesBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureFebria ArmaNo ratings yet
- GD in PregnancyDocument37 pagesGD in Pregnancymohammed makkiNo ratings yet
- Hyperthyroidism in Pregnancy: Jorge H. MDDocument23 pagesHyperthyroidism in Pregnancy: Jorge H. MDRashid HussainNo ratings yet
- Thyroid Disorders During Pregnancy and A PDFDocument6 pagesThyroid Disorders During Pregnancy and A PDFtania jannah100% (1)
- Thyroid Disease in PregnancyDocument12 pagesThyroid Disease in PregnancyOldriana Prawiro HapsariNo ratings yet
- Thyroid StormDocument36 pagesThyroid StormSabrina ShalhoutNo ratings yet
- Hyperthyroidism and Thyrotoxicosis PDFDocument16 pagesHyperthyroidism and Thyrotoxicosis PDFMuhammad IkbarNo ratings yet
- Pathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis)Document31 pagesPathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis)Juan Sebastian Carrillo GomezNo ratings yet
- Akibat Pada Kehamilan Akibat Pada KehamilanDocument4 pagesAkibat Pada Kehamilan Akibat Pada KehamilanTrisnawanta Asih PasamboNo ratings yet
- PIIS2214623714000295Document6 pagesPIIS2214623714000295Ita MaghfirahNo ratings yet
- ThyroidDocument31 pagesThyroidAmmar HattemNo ratings yet
- Graves Disease - StatPearls - NCBI BookshelfDocument8 pagesGraves Disease - StatPearls - NCBI BookshelfDr.Pradip PatilNo ratings yet
- Wo Week 4 (Hyperthyroidism)Document12 pagesWo Week 4 (Hyperthyroidism)Theddyon BhenlieNo ratings yet
- Bening Disease of Thyroid GlandDocument85 pagesBening Disease of Thyroid GlandKarishma MishraNo ratings yet
- PDF document-CD8968C1BAE7-1Document22 pagesPDF document-CD8968C1BAE7-1Sean SialanaNo ratings yet
- Pregnancy Thyroid DiseaseDocument8 pagesPregnancy Thyroid DiseaseYhang Lidi TamaNo ratings yet
- 10 Hyperthyroidism in Pregnancy: Jorge H. MestmanDocument22 pages10 Hyperthyroidism in Pregnancy: Jorge H. MestmanRashid HussainNo ratings yet
- Thyroid Physiology and Common Diseases in Pregnancy: Review of LiteratureDocument8 pagesThyroid Physiology and Common Diseases in Pregnancy: Review of LiteratureMarijeimy Alejandra Ortíz FerroNo ratings yet
- Thyroid Disorders in PregnancyDocument3 pagesThyroid Disorders in PregnancyZoel Nikonian100% (1)
- Hipotiroidism Diaz 2014Document17 pagesHipotiroidism Diaz 2014Achmad ArrizalNo ratings yet
- Types: HyperthyroidismDocument12 pagesTypes: HyperthyroidismArunNo ratings yet
- Hyperthyroidism Article PubmedDocument12 pagesHyperthyroidism Article PubmedSandu AlexandraNo ratings yet
- Atow 496 00 01Document9 pagesAtow 496 00 01Nguyen Ngoc ChungNo ratings yet
- Thyroid StormDocument11 pagesThyroid StormAndrew UtamaNo ratings yet
- Hyperthyroidism: Sudiarto, MNDocument21 pagesHyperthyroidism: Sudiarto, MNerikaNo ratings yet
- 1 2 3 4 MergedDocument20 pages1 2 3 4 Mergedcataleya mesaNo ratings yet
- Hyperthyroidism and Thyrotoxicosis: Practice EssentialsDocument39 pagesHyperthyroidism and Thyrotoxicosis: Practice Essentialssyl viNo ratings yet
- [1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancyDocument8 pages[1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancyClaudia IrimieNo ratings yet
- Background: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureDocument8 pagesBackground: Excessive Release of Thyroid Hormones (THS) Hypertension Congestive Heart FailureIkmal HazliNo ratings yet
- American Thyroid Association Guidelines For Detection of Thyroid DysfunctionDocument5 pagesAmerican Thyroid Association Guidelines For Detection of Thyroid DysfunctionUdsanee SukpimonphanNo ratings yet
- Therapeutic Approach of Fetal Thyroid Disorders: Research inDocument5 pagesTherapeutic Approach of Fetal Thyroid Disorders: Research inAlma Veronica Gonzalez SandovalNo ratings yet
- ThyroidDocument12 pagesThyroidrpjaymaNo ratings yet
- Diabetes and Thyroid Disease A Common Association With Clinical ConsequencesDocument4 pagesDiabetes and Thyroid Disease A Common Association With Clinical Consequenceseliana suxoNo ratings yet
- Hyperthyroidism and Thyrotoxicosis - Practice Essentials, Background, PathophysiologyDocument13 pagesHyperthyroidism and Thyrotoxicosis - Practice Essentials, Background, Pathophysiologyabenezer g/kirstosNo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument11 pagesBest Practice & Research Clinical Endocrinology & MetabolismGLORIA ANDREA ORJUELA FLOREZNo ratings yet
- Jurnal Hipertiroid KehamilanDocument5 pagesJurnal Hipertiroid KehamilanAbdurrohman IzzuddinNo ratings yet
- Hyperthyroidism in Childhood: Causes, When and How To Treat: ReviewDocument7 pagesHyperthyroidism in Childhood: Causes, When and How To Treat: ReviewarthoclaseNo ratings yet
- Laboratory Assesment of Thyroid Function PMC2003Document14 pagesLaboratory Assesment of Thyroid Function PMC2003Muhammad Dadan KurniawanNo ratings yet
- Thyroid Diet: How to Improve Thyroid Disorders, Manage Thyroid Symptoms, Lose Weight, and Improve Your Metabolism through Diet!From EverandThyroid Diet: How to Improve Thyroid Disorders, Manage Thyroid Symptoms, Lose Weight, and Improve Your Metabolism through Diet!No ratings yet
- Hashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Vanschalkwyk2015 VV PDFDocument9 pagesVanschalkwyk2015 VV PDFAulia RahmaNo ratings yet
- Diagnosis, Elevation and ManagementDocument23 pagesDiagnosis, Elevation and ManagementFcv Asvira AnisNo ratings yet
- ACOG Guides and Opinion On Placenta Accreta ManagementDocument5 pagesACOG Guides and Opinion On Placenta Accreta ManagementCharlene FernándezNo ratings yet
- Poon and Nikolaides 2014Document12 pagesPoon and Nikolaides 2014Rosália Coutada0% (1)
- Imaging of Adenxal Masses in Pregnancy PDFDocument15 pagesImaging of Adenxal Masses in Pregnancy PDFRosália CoutadaNo ratings yet
- Review Adnexal Masses Pregnancy Rcog PDFDocument6 pagesReview Adnexal Masses Pregnancy Rcog PDFRosália Coutada100% (1)
- Physiological Changes in PregnancyDocument40 pagesPhysiological Changes in PregnancyArhum SiddiqiNo ratings yet
- KIEHN Silphion Multis Iam Annis in Ea Terra Non Invenitur The Extintion of SilphiumDocument9 pagesKIEHN Silphion Multis Iam Annis in Ea Terra Non Invenitur The Extintion of SilphiumPablo Varona RubioNo ratings yet
- MK Polyhydramnios and Oligohydramnios (OBGY)Document14 pagesMK Polyhydramnios and Oligohydramnios (OBGY)Moses Jr KazevuNo ratings yet
- Physiology of Menstruation: TH THDocument7 pagesPhysiology of Menstruation: TH THRainy DaysNo ratings yet
- Women Wellness CourseDocument69 pagesWomen Wellness CourseEktarayogaNo ratings yet
- G7 Summative Test For LAS 5 8Document2 pagesG7 Summative Test For LAS 5 8Meralyn Puaque BustamanteNo ratings yet
- Twins and MFPDocument6 pagesTwins and MFPNoha AkramNo ratings yet
- Drugs in Pregnancy: A Handbook For Pharmacists and PhysiciansDocument3 pagesDrugs in Pregnancy: A Handbook For Pharmacists and PhysiciansSeno Adi WicaksonoNo ratings yet
- Case Scenario NCPDocument2 pagesCase Scenario NCPDarwin QuirimitNo ratings yet
- Ambiguous GenitaliaDocument2 pagesAmbiguous Genitaliamimit sasmitaNo ratings yet
- Engineering Design An Introduction 2nd Edition Karsnitz Test Bank Full Chapter PDFDocument36 pagesEngineering Design An Introduction 2nd Edition Karsnitz Test Bank Full Chapter PDFRobertFordicwr100% (13)
- Hyperthyroidism Vs HypothyroidismDocument12 pagesHyperthyroidism Vs Hypothyroidismazizan hannyNo ratings yet
- Task 3 Xblaw PoeDocument4 pagesTask 3 Xblaw PoeMbalenhle NdlovuNo ratings yet
- The Lack of Job Opportunities Is Also One of The Main Reasons Why Many Filipinos Are Forced To Seek Greener Pastures AbroadDocument2 pagesThe Lack of Job Opportunities Is Also One of The Main Reasons Why Many Filipinos Are Forced To Seek Greener Pastures AbroadLouise Gabrielle CadenasNo ratings yet
- UTERINE ATONY - CASE STUDY - EditedDocument50 pagesUTERINE ATONY - CASE STUDY - EditedMonica BorjaNo ratings yet
- NBME 14 - AnswersDocument208 pagesNBME 14 - Answersmerontesfaye51No ratings yet
- Principles of Physical AssessmentDocument58 pagesPrinciples of Physical AssessmentAnna Fayeziah YussophNo ratings yet
- NCM 209 Rle-Dr RotationDocument15 pagesNCM 209 Rle-Dr RotationShan LabajoNo ratings yet
- Mammography: What Is The Goal of Mammography?Document13 pagesMammography: What Is The Goal of Mammography?jeron encaboNo ratings yet
- Domperidone For Increasing Breast Milk Supply 260219 PDFDocument2 pagesDomperidone For Increasing Breast Milk Supply 260219 PDFANneNo ratings yet
- BJAS (Volume 4 Issue 1)Document159 pagesBJAS (Volume 4 Issue 1)Tshegay NorbuNo ratings yet
- ADRI USG KoasDocument108 pagesADRI USG KoasFirza FatchyaNo ratings yet
- Newborn ReflexesDocument3 pagesNewborn Reflexesabayaivyliana25No ratings yet
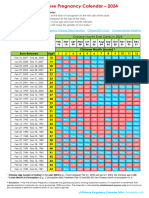
- Chinese Pregnancy Chart 2024Document1 pageChinese Pregnancy Chart 2024crisgel.121100No ratings yet
- Product Guide 9th - SPLDocument353 pagesProduct Guide 9th - SPLrajib paulNo ratings yet
- Hubungan Dukungan Suami Terhadap Tingkat Kecemasan Ibu Hamil Menjelang Persalinan Di Ruang Persalinan Rumah Sakit Umum Daerah Karanganyar Tahun 2017Document10 pagesHubungan Dukungan Suami Terhadap Tingkat Kecemasan Ibu Hamil Menjelang Persalinan Di Ruang Persalinan Rumah Sakit Umum Daerah Karanganyar Tahun 2017DianNo ratings yet
- 2015 Clinical Practice Guidelines On Obstetric and Gynecologic Infectious DiseasesDocument59 pages2015 Clinical Practice Guidelines On Obstetric and Gynecologic Infectious DiseasesSaint Pauls ObgynNo ratings yet
- Kunyit Asam Terhadap Intensitas Nyeri Haid 1Document5 pagesKunyit Asam Terhadap Intensitas Nyeri Haid 1Yanna SailanyNo ratings yet
- Labour Class NoteDocument7 pagesLabour Class NoteCarzo ParazzoNo ratings yet
- Management of Miscarriage and Sepsis: EsmoeDocument29 pagesManagement of Miscarriage and Sepsis: EsmoeLana LocoNo ratings yet















































![[1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancy](https://imgv2-2-f.scribdassets.com/img/document/552054434/149x198/0ad7f435ea/1710545307?v=1)