You might also like
- How Food Handlers Can Spread IllnessDocument2 pagesHow Food Handlers Can Spread IllnessSavitri Maharani BudimanNo ratings yet
- NTCP Adult TB Guidelines 27.5.2014Document120 pagesNTCP Adult TB Guidelines 27.5.2014Savitri Maharani BudimanNo ratings yet
- TB Nutrition Care GuidelinesDocument2 pagesTB Nutrition Care GuidelinesSavitri Maharani BudimanNo ratings yet
- PDF File PDFDocument9 pagesPDF File PDFSavitri Maharani BudimanNo ratings yet
- Immunological Manifestation of Extra Pulmonary TBDocument4 pagesImmunological Manifestation of Extra Pulmonary TBSavitri Maharani BudimanNo ratings yet
- TB Nutrition Care GuidelinesDocument2 pagesTB Nutrition Care GuidelinesSavitri Maharani BudimanNo ratings yet
- Bmi Asia Strategies PDFDocument7 pagesBmi Asia Strategies PDFHevi NetyaNo ratings yet
- Abdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduDocument4 pagesAbdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduSavitri Maharani BudimanNo ratings yet
- Breakfast ConsumptionDocument2 pagesBreakfast ConsumptionSavitri Maharani BudimanNo ratings yet
- TB Nutrition Care GuidelinesDocument2 pagesTB Nutrition Care GuidelinesSavitri Maharani BudimanNo ratings yet
- SNI 01-3820-1995 Sosis DagingDocument0 pagesSNI 01-3820-1995 Sosis DagingDanu WijanarkoNo ratings yet
- Eating Well For Your Burn Injury: How To Find UsDocument2 pagesEating Well For Your Burn Injury: How To Find UsSavitri Maharani BudimanNo ratings yet
- PGRS 2014Document165 pagesPGRS 2014Rizky Arifandy75% (8)
- Skipper ArticleDocument10 pagesSkipper ArticleSavitri Maharani BudimanNo ratings yet
- S 1368980007000389 ADocument8 pagesS 1368980007000389 ASavitri Maharani BudimanNo ratings yet
- AdaDocument192 pagesAdaSavitri Maharani BudimanNo ratings yet
- Association Between Fruits and Vegetables Intake and Frequency of Breakfast and Snacks Consumption A Cross-Sectional StudyDocument21 pagesAssociation Between Fruits and Vegetables Intake and Frequency of Breakfast and Snacks Consumption A Cross-Sectional StudySavitri Maharani BudimanNo ratings yet
- Reducing Your Risk of Stroke: Don't Wait For It To Happen To YouDocument8 pagesReducing Your Risk of Stroke: Don't Wait For It To Happen To YouSavitri Maharani BudimanNo ratings yet
- Eating PatternDocument27 pagesEating PatternSavitri Maharani BudimanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Tools of Titans by Tim Ferriss - Book Summary & PDFDocument15 pagesTools of Titans by Tim Ferriss - Book Summary & PDFVikram100% (1)
- Biological Theories of AgingDocument29 pagesBiological Theories of AgingdulceRN67% (3)
- Biocom Price List for Supplements, Water Filters, Cleaning Products and MoreDocument2 pagesBiocom Price List for Supplements, Water Filters, Cleaning Products and MoreChristian HaldenWangNo ratings yet
- Fiji Honey HarvestingDocument26 pagesFiji Honey HarvestingJohnCaldeiraNo ratings yet
- Nutritioncalc Plus ReportDocument1 pageNutritioncalc Plus Reportapi-266108494No ratings yet
- AE1 LISTENING EXAMDocument2 pagesAE1 LISTENING EXAMPhước LưuNo ratings yet
- Material Balance Laboratory: Ice Cream Process III. Equipment: IV. MaterialsDocument5 pagesMaterial Balance Laboratory: Ice Cream Process III. Equipment: IV. MaterialsMaurice HadawayNo ratings yet
- Innocenti Declaration 1990Document2 pagesInnocenti Declaration 1990ANDREASNo ratings yet
- Exploring Debate 1 Word ListDocument20 pagesExploring Debate 1 Word ListKwangyim LeeNo ratings yet
- Healthy EatingDocument2 pagesHealthy EatingMissdiary RahmanNo ratings yet
- Dayna Ross: ObjectiveDocument2 pagesDayna Ross: ObjectiveDayna RossNo ratings yet
- The Key Difference Between Essential and NonDocument2 pagesThe Key Difference Between Essential and NonRafael CurtesNo ratings yet
- Mens Fitness Guide Meals That Make Muscle 2nd Edition 2020Document68 pagesMens Fitness Guide Meals That Make Muscle 2nd Edition 2020ginoNo ratings yet
- SamplingDocument41 pagesSamplingShailendra DhakadNo ratings yet
- Lipids - FatsDocument13 pagesLipids - FatsJohn Jill T. VillamorNo ratings yet
- The Broste Group Corporate PresentationDocument28 pagesThe Broste Group Corporate Presentation111384No ratings yet
- SURGICAL NUTRITION GUIDEDocument59 pagesSURGICAL NUTRITION GUIDEPrincewill SeiyefaNo ratings yet
- Counsels On Diet and Foods PDFDocument507 pagesCounsels On Diet and Foods PDFvitorcruz7100% (2)
- Farm2Fam Success Story - Live Microgreens To Keep You HealthyDocument8 pagesFarm2Fam Success Story - Live Microgreens To Keep You HealthyShubham KumarNo ratings yet
- Group 1 Kamias Candy Product PitchingDocument13 pagesGroup 1 Kamias Candy Product PitchingCHAMS Elementary DepartmentNo ratings yet
- Dietary Guidelines Allowances For Americans 2010 USDADocument112 pagesDietary Guidelines Allowances For Americans 2010 USDAkiki_scrabsNo ratings yet
- Hope 3 Q2 M9Document16 pagesHope 3 Q2 M9lalatina best grillNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
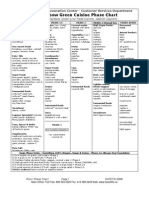
- Summary of Rainbow Green Cuisine PhasesDocument2 pagesSummary of Rainbow Green Cuisine Phasesjmac64100% (1)
- Physical Health and Mental HealthDocument2 pagesPhysical Health and Mental HealthLuise MauieNo ratings yet
- UHT 1 Kelas 9 Semester 1 2011 2012Document4 pagesUHT 1 Kelas 9 Semester 1 2011 2012Tri Wahyuningsih100% (1)
- Level 1 v4 Forms PG 1-9Document9 pagesLevel 1 v4 Forms PG 1-9Jože MajcenNo ratings yet
- SEMINAR ON OSTEOMALACIA CAUSES AND SYMPTOMSDocument24 pagesSEMINAR ON OSTEOMALACIA CAUSES AND SYMPTOMSSheela Raja KumariNo ratings yet
- European Confessions of Moorish ExistenceDocument15 pagesEuropean Confessions of Moorish Existencetbelote796% (27)
- McLeod's Daughters stars catch up after 11 yearsDocument2 pagesMcLeod's Daughters stars catch up after 11 yearsMartina MarićNo ratings yet