You might also like
- Vanschalkwyk2015 VV PDFDocument9 pagesVanschalkwyk2015 VV PDFAulia RahmaNo ratings yet
- ACOG Guides and Opinion On Placenta Accreta ManagementDocument5 pagesACOG Guides and Opinion On Placenta Accreta ManagementCharlene FernándezNo ratings yet
- Diagnosis, Elevation and ManagementDocument23 pagesDiagnosis, Elevation and ManagementFcv Asvira AnisNo ratings yet
- Poon and Nikolaides 2014Document12 pagesPoon and Nikolaides 2014Rosália Coutada0% (1)
- TiroideDocument10 pagesTiroideRosália CoutadaNo ratings yet
- Managing Adnexal Masses in PregnancyDocument6 pagesManaging Adnexal Masses in PregnancyRosália Coutada100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Definition of TermsDocument2 pagesDefinition of TermsjennahNo ratings yet
- Risk Factors for Low Birth Weight in MalaysiaDocument5 pagesRisk Factors for Low Birth Weight in Malaysiaerine5995No ratings yet
- Final Dissertation - Sharma AditiDocument180 pagesFinal Dissertation - Sharma AditiManish KumarNo ratings yet
- Science 5 DLP 3 - PubertyDocument8 pagesScience 5 DLP 3 - PubertyMark Cua100% (4)
- Instruments for Exams and Procedures in OBGYNDocument12 pagesInstruments for Exams and Procedures in OBGYNJennyDaniel100% (1)
- Female Reproductive System: Related Kidshealth LinksDocument7 pagesFemale Reproductive System: Related Kidshealth Linksrichy0% (1)
- Incomplete Abortion MINI CASE STUDY (Group 3)Document22 pagesIncomplete Abortion MINI CASE STUDY (Group 3)Twobee Evelyn Claire62% (21)
- Hubungan Malnutrisi Dengan Kejadian Dismenorea Pada Remaja Putri Di Sman 1 Kampar TAHUN 2014Document8 pagesHubungan Malnutrisi Dengan Kejadian Dismenorea Pada Remaja Putri Di Sman 1 Kampar TAHUN 2014Cita Reast Wulansari83No ratings yet
- MaternalDocument5 pagesMaternalStephanie Joy EscalaNo ratings yet
- Ceftriaxone, Misoprostol, OxytocinDocument4 pagesCeftriaxone, Misoprostol, OxytocinKrizia Bonilla100% (1)
- JKS Vol 11 No 1 April 2023 Hal 71-79Document9 pagesJKS Vol 11 No 1 April 2023 Hal 71-79Linny Aswita SariNo ratings yet
- Bio Trifold PamphletDocument2 pagesBio Trifold Pamphletapi-286071688No ratings yet
- Anatomi Reproduksi WanitaDocument23 pagesAnatomi Reproduksi WanitaocepNo ratings yet
- 02 - IRAOvulation Induction For TheDocument11 pages02 - IRAOvulation Induction For TheHartanto LieNo ratings yet
- Pi Is 0015028208033050Document17 pagesPi Is 0015028208033050Annisa YutamiNo ratings yet
- OB1 3.3A Normal Puerperium and Puerperal FeverDocument7 pagesOB1 3.3A Normal Puerperium and Puerperal FeverManjulaNo ratings yet
- Cabbage Leaves Effective in Reducing Breast Milk DamsDocument6 pagesCabbage Leaves Effective in Reducing Breast Milk DamsAmeliarNo ratings yet
- New Developments in The Medical & Surgical Therapy For FibroidsDocument20 pagesNew Developments in The Medical & Surgical Therapy For FibroidsernestosandNo ratings yet
- Preterm Labour and PROMDocument25 pagesPreterm Labour and PROMNinaNo ratings yet
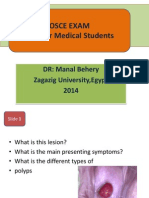
- OSCE in Obstetrics&Gynecology For UndergraduateDocument66 pagesOSCE in Obstetrics&Gynecology For UndergraduateManal Behery80% (5)
- VaginaDocument1 pageVaginaEusebiu LambruNo ratings yet
- Cardiovascular Disorders and PregnancyDocument31 pagesCardiovascular Disorders and PregnancyChari RivoNo ratings yet
- UroginDocument13 pagesUroginShandy Suwanto PutraNo ratings yet
- Mullerian Duct Abnormalities, Hirsutism, Bacterial Vaginosis & IUCDsDocument4 pagesMullerian Duct Abnormalities, Hirsutism, Bacterial Vaginosis & IUCDsrohitNo ratings yet
- Knowledge of nursing students on polycystic ovarian syndromeDocument80 pagesKnowledge of nursing students on polycystic ovarian syndromeDiksh JindeNo ratings yet
- Pharmacology of Drugs Acting On Uterus - MBBSDocument23 pagesPharmacology of Drugs Acting On Uterus - MBBSDr.U.P.Rathnakar.MD.DIH.PGDHM100% (5)
- Module 5 Enrichment TaskDocument1 pageModule 5 Enrichment TaskAngelyn CayabanNo ratings yet
- Ob Talking Points Efm:: W.I.N.KDocument4 pagesOb Talking Points Efm:: W.I.N.KRon ChurrascoNo ratings yet
- Caesarean Scar Ectopic Pregnancy: Case ReportDocument3 pagesCaesarean Scar Ectopic Pregnancy: Case ReportDewi SaftariNo ratings yet
- Assessment of A Pregnant FamilyDocument4 pagesAssessment of A Pregnant FamilyLuna Sang-anNo ratings yet