You might also like
- KomDocument8 pagesKomGeorge Herland PradiktaNo ratings yet
- KomDocument8 pagesKomGeorge Herland PradiktaNo ratings yet
- YrtyrtDocument1 pageYrtyrtGeorge Herland PradiktaNo ratings yet
- WWWDocument1 pageWWWGeorge Herland PradiktaNo ratings yet
- Opioid Pharmacology: Pain Physician 2008: Opioid Special Issue: 11: S133-S153 - ISSN 1533-3159Document22 pagesOpioid Pharmacology: Pain Physician 2008: Opioid Special Issue: 11: S133-S153 - ISSN 1533-3159Suresh KumarNo ratings yet
- EeeDocument1 pageEeeGeorge Herland PradiktaNo ratings yet
- RRRHJKKHDocument1 pageRRRHJKKHGeorge Herland PradiktaNo ratings yet
- ZXCDocument1 pageZXCGeorge Herland PradiktaNo ratings yet
- Jbsi 18 NXJPW 0 U 1Document1 pageJbsi 18 NXJPW 0 U 1George Herland PradiktaNo ratings yet
- BBBDocument1 pageBBBGeorge Herland PradiktaNo ratings yet
- JNC 7 (Klasifikasi Hipertensi) PDFDocument2 pagesJNC 7 (Klasifikasi Hipertensi) PDFAbdur RahmanNo ratings yet
- Googles BookDocument1 pageGoogles BookGeorge Herland PradiktaNo ratings yet
- Popo PopDocument1 pagePopo PopGeorge Herland PradiktaNo ratings yet
- Serial NoDocument1 pageSerial NoGeorge Herland PradiktaNo ratings yet
- Read Me 1Document10 pagesRead Me 1pmk888No ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- EulaDocument63 pagesEulatechkasambaNo ratings yet
- List FileDocument73 pagesList FileGeorge Herland PradiktaNo ratings yet
- Accidental Radioactive ContaminationDocument1 pageAccidental Radioactive ContaminationGeorge Herland PradiktaNo ratings yet
- List FileDocument73 pagesList FileGeorge Herland PradiktaNo ratings yet
- Jurnal VertebraDocument10 pagesJurnal VertebraGeorge Herland PradiktaNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Syllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsDocument6 pagesSyllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsOEAENo ratings yet
- Acute Tracheobronchitis Causes, Symptoms, TreatmentDocument2 pagesAcute Tracheobronchitis Causes, Symptoms, TreatmentNicole Shannon CariñoNo ratings yet
- JUSTINE Medical-for-Athletes-2-1Document2 pagesJUSTINE Medical-for-Athletes-2-1joselito papa100% (1)
- As 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesDocument8 pagesAs 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesSAI Global - APACNo ratings yet
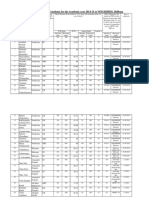
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNo ratings yet
- Appendix - 6 - Site Logistics PlanDocument16 pagesAppendix - 6 - Site Logistics PlanRamesh BabuNo ratings yet
- Anarchy RPG 0.2 Cover 1 PDFDocument14 pagesAnarchy RPG 0.2 Cover 1 PDFanon_865633295No ratings yet
- Weeblylp MedicinaDocument18 pagesWeeblylp Medicinaapi-538325537No ratings yet
- The Process of Grief PDFDocument6 pagesThe Process of Grief PDFnicoletagr2744100% (1)
- Handbook of Laboratory Animal Science - Vol IIIDocument319 pagesHandbook of Laboratory Animal Science - Vol IIICarlos AlmeidaNo ratings yet
- Chapter 22 The First Heart SoundDocument5 pagesChapter 22 The First Heart SoundAbhilash ReddyNo ratings yet
- Facts of MaintenanceDocument9 pagesFacts of Maintenancegeorge youssefNo ratings yet
- OCPD: Symptoms, Diagnosis and TreatmentDocument4 pagesOCPD: Symptoms, Diagnosis and TreatmentRana Muhammad Ahmad Khan ManjNo ratings yet
- Introduction 1 Esoteric HealingDocument20 pagesIntroduction 1 Esoteric HealingChicowski Caires100% (1)
- Swan-Ganz Catheter Insertion GuideDocument3 pagesSwan-Ganz Catheter Insertion GuideJoshNo ratings yet
- LabTec Product SpecificationsDocument292 pagesLabTec Product SpecificationsDiego TobrNo ratings yet
- Nursing Interventions for Ineffective Airway ClearanceDocument3 pagesNursing Interventions for Ineffective Airway Clearanceaurezea100% (3)
- EN Sample Paper 12 UnsolvedDocument9 pagesEN Sample Paper 12 Unsolvedguptasubhanjali21No ratings yet
- Injeksi Mecobalamin Vas ScoreDocument5 pagesInjeksi Mecobalamin Vas ScoreHerdy ArshavinNo ratings yet
- College Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeDocument12 pagesCollege Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeGlennKesslerWP100% (1)
- (260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPDocument43 pages(260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPreginaNo ratings yet
- Detailed Advertisement of Various GR B & C 2023 - 0 PDFDocument47 pagesDetailed Advertisement of Various GR B & C 2023 - 0 PDFMukul KostaNo ratings yet
- Occlusion For Implant Suppported CDDocument4 pagesOcclusion For Implant Suppported CDpopat78No ratings yet
- Cough and ColdsDocument3 pagesCough and ColdsKarl-Ren Lacanilao100% (1)
- Labcorp: Patient ReportDocument4 pagesLabcorp: Patient ReportAsad PrinceNo ratings yet
- Leaving Disasters Behind: A Guide To Disaster Risk Reduction in EthiopiaDocument12 pagesLeaving Disasters Behind: A Guide To Disaster Risk Reduction in EthiopiaOxfamNo ratings yet
- Dr. Abazar Habibinia's Guide to Overweight, Obesity, and Weight ManagementDocument41 pagesDr. Abazar Habibinia's Guide to Overweight, Obesity, and Weight ManagementTasniiem KhmbataNo ratings yet
- 798 3072 1 PBDocument12 pages798 3072 1 PBMariana RitaNo ratings yet
- Environmental Hazards For The Nurse As A Worker - Nursing Health, & Environment - NCBI Bookshelf PDFDocument6 pagesEnvironmental Hazards For The Nurse As A Worker - Nursing Health, & Environment - NCBI Bookshelf PDFAgung Wicaksana100% (1)
- Updates On Upper Eyelid Blepharoplasty.4Document8 pagesUpdates On Upper Eyelid Blepharoplasty.4Dimitris RodriguezNo ratings yet