You might also like
- Labor Cost Code PDFDocument5 pagesLabor Cost Code PDFkarthikaswiNo ratings yet
- Free HR Incident Investigation FormDocument2 pagesFree HR Incident Investigation FormRichard R M ThodéNo ratings yet
- Version 1 - January 2015: Makati City, PhilippinesDocument64 pagesVersion 1 - January 2015: Makati City, PhilippinesRiann VistoNo ratings yet
- Human Resource ManagementDocument15 pagesHuman Resource ManagementAditiNo ratings yet
- F.hr.03 Training PlanDocument14 pagesF.hr.03 Training PlanSaurabhNo ratings yet
- Guidelines PipDocument3 pagesGuidelines Pipsimee25No ratings yet
- At2 4Document2 pagesAt2 4Rago RamsNo ratings yet
- Sample Only: Competency-Based Standards For Rank-and-File Employees Assessment ToolDocument2 pagesSample Only: Competency-Based Standards For Rank-and-File Employees Assessment ToolJerry Barad SarioNo ratings yet
- Project Staffing Plan: Document Revision/Release StatusDocument7 pagesProject Staffing Plan: Document Revision/Release StatusAnurag SrivastavaNo ratings yet
- RPSG Management Task Tracker Ver 1.0.1 28 Oct 19Document1 pageRPSG Management Task Tracker Ver 1.0.1 28 Oct 19Rocky BisNo ratings yet
- Annual Training Calendar 2011-2012Document10 pagesAnnual Training Calendar 2011-2012krovvidiprasadaraoNo ratings yet
- 1training Proposal Format - New FormatDocument46 pages1training Proposal Format - New FormatKrasne MladyNo ratings yet
- IC HR Dashboard1Document16 pagesIC HR Dashboard1barakkat72No ratings yet
- Rapid Plant Assessment: Table 3 - Tour DataDocument3 pagesRapid Plant Assessment: Table 3 - Tour Datapratip064149No ratings yet
- Performance Management and ReviewDocument5 pagesPerformance Management and ReviewShravanti Das0% (1)
- 02.c.d.e.f.h.induction and Orientation PolicyDocument7 pages02.c.d.e.f.h.induction and Orientation PolicyArjun Bhanot100% (1)
- Company Name Skill Matrix: Scoring Criteria 9-10 Outstanding 7-8 Excellent 5-6 Good 3-4 Average 1-2 PoorDocument1 pageCompany Name Skill Matrix: Scoring Criteria 9-10 Outstanding 7-8 Excellent 5-6 Good 3-4 Average 1-2 PoorKodamShruthiNo ratings yet
- PERFORMANCE EVALUATIONDocument4 pagesPERFORMANCE EVALUATIONclifford alejoNo ratings yet
- The Most Important Roles For Your PPM: PPM Role PPM Responsibility Typical Organizational Role Your NotesDocument2 pagesThe Most Important Roles For Your PPM: PPM Role PPM Responsibility Typical Organizational Role Your NotesMarielle MaltoNo ratings yet
- Interview Form HCADocument4 pagesInterview Form HCAThabo NkomoNo ratings yet
- Logic Model Grant Workplan GuidelinesDocument10 pagesLogic Model Grant Workplan GuidelinesPrincess SonalNo ratings yet
- SMILE On BoardingDocument14 pagesSMILE On Boardingrhodalyn dionesio100% (1)
- Annual Employee Self-ReviewDocument4 pagesAnnual Employee Self-ReviewafiqruslanNo ratings yet
- Waterfall Large LC QuickRef v1.2Document1 pageWaterfall Large LC QuickRef v1.2Swarup NakkaNo ratings yet
- 04 SOP GROOMING - UpdateDocument6 pages04 SOP GROOMING - UpdateSiti Rainy SyamNo ratings yet
- OBM Level I OBM Level II Obm Level Iii Application Category Process Analysis QuestionsDocument24 pagesOBM Level I OBM Level II Obm Level Iii Application Category Process Analysis QuestionsFeras AlswairkyNo ratings yet
- External and Internal Transfer ProcessDocument18 pagesExternal and Internal Transfer Processshadi alshadafanNo ratings yet
- Calculate Training and Operating Costs with this Free Online CalculatorDocument1 pageCalculate Training and Operating Costs with this Free Online CalculatorRoosy RoosyNo ratings yet
- Build a Budget with this Monthly PlannerDocument7 pagesBuild a Budget with this Monthly Plannerkisan singhNo ratings yet
- Liaison OfficerDocument3 pagesLiaison OfficerMaria Cristina ItaoNo ratings yet
- Training PolicyDocument6 pagesTraining Policygaza222No ratings yet
- Contractor Performance Evaluation QuestionnaireDocument15 pagesContractor Performance Evaluation Questionnaireraahul_nNo ratings yet
- Performance Review Template (Self, Manager, Peers)Document10 pagesPerformance Review Template (Self, Manager, Peers)Marko IllustrisimoNo ratings yet
- Credential IngDocument13 pagesCredential Ingdr_rajatjainNo ratings yet
- PTO PolicyDocument5 pagesPTO PolicyMan Tue Thai100% (1)
- Project-Selection-Tool v3.5Document12 pagesProject-Selection-Tool v3.5rgrao85No ratings yet
- Ba 420 Update Career Development PlanDocument4 pagesBa 420 Update Career Development Planapi-312991699No ratings yet
- Performance Improvement (PI) Plan and Template: Health Care Association of New JerseyDocument46 pagesPerformance Improvement (PI) Plan and Template: Health Care Association of New JerseyRógini HaasNo ratings yet
- Recruitment Manager: Simple EffectiveDocument14 pagesRecruitment Manager: Simple EffectiveSaw PreciousNo ratings yet
- Expense Claim Form: March 2018-Feb 2019Document1 pageExpense Claim Form: March 2018-Feb 2019Varun SirohiNo ratings yet
- Presented by Celia BandelierDocument54 pagesPresented by Celia BandelierCharmee Jane Lozano PadillaNo ratings yet
- Sample Goals ListDocument29 pagesSample Goals ListSurajit MitraNo ratings yet
- Staff Development: A Process for Improving Teaching and LearningDocument5 pagesStaff Development: A Process for Improving Teaching and Learning1baba2No ratings yet
- Check Out The Original Dashboard by Mynda Treacy Here: Https://Youtu - Be/Rsx43G7Tbbs Check Out The Original Dashboard by HereDocument31 pagesCheck Out The Original Dashboard by Mynda Treacy Here: Https://Youtu - Be/Rsx43G7Tbbs Check Out The Original Dashboard by HereAndi Purnomo100% (1)
- Reference checking templateDocument3 pagesReference checking templateEnza R100% (1)
- Public Events Calendar: JANUARY 2022 February 2022 MARCH 2022Document2 pagesPublic Events Calendar: JANUARY 2022 February 2022 MARCH 2022Afiq AazmiNo ratings yet
- QA: 5S Improvement Techniques: Contributing To The Application of Workplace Organisation TechniquesDocument58 pagesQA: 5S Improvement Techniques: Contributing To The Application of Workplace Organisation TechniquesRashid GhaniNo ratings yet
- Objective Weightage KPI Weightage Q1 Q2 Q3 Q4: Operational EfficiencyDocument2 pagesObjective Weightage KPI Weightage Q1 Q2 Q3 Q4: Operational EfficiencyOsama FaridNo ratings yet
- PolicyDocument20 pagesPolicyPranay DasNo ratings yet
- Juniper Networks Employee Benefits GuideDocument3 pagesJuniper Networks Employee Benefits GuideYerragola PrakashNo ratings yet
- Ski Incident Investigation ToolDocument10 pagesSki Incident Investigation ToolsantuchetuNo ratings yet
- KPI Scorecard Template Tracks Company Goals and ObjectivesDocument2 pagesKPI Scorecard Template Tracks Company Goals and ObjectivesStella Giovanna MartínezNo ratings yet
- Performance Appraisal Form For HRDocument5 pagesPerformance Appraisal Form For HRAmmarah KaleemNo ratings yet
- Salary CalculatorDocument19 pagesSalary Calculatorvirag_shahsNo ratings yet
- Manpower Request FormDocument1 pageManpower Request FormPragathishNo ratings yet
- Daily Cleaning ChecklistDocument1 pageDaily Cleaning ChecklistDa Vou DNo ratings yet
- Standard Org Chart & Role DescriptionsDocument15 pagesStandard Org Chart & Role DescriptionsYoung-seok HwangNo ratings yet
- Major Oroject On Management Information SystemDocument48 pagesMajor Oroject On Management Information SystemAbhimanyuGulatiNo ratings yet
- BEAMANAL - Single & Continuous Beam AnalysisDocument6 pagesBEAMANAL - Single & Continuous Beam AnalysistambokNo ratings yet
- S Curve WhitepaperDocument6 pagesS Curve WhitepaperSana SanNo ratings yet
- Book S Curve For Construction Sample Excel Bing PDFDocument4 pagesBook S Curve For Construction Sample Excel Bing PDFmy.nafi.pmp5283No ratings yet
- Business Analysis Solution Options TemplateDocument3 pagesBusiness Analysis Solution Options Templatemy.nafi.pmp5283No ratings yet
- Cashflow TemplateDocument4 pagesCashflow Templatesukma nurhidayatNo ratings yet
- 14 Steps To Create Cash Flow FR PDFDocument14 pages14 Steps To Create Cash Flow FR PDFmy.nafi.pmp5283No ratings yet
- Benefit-Cost AnalysisDocument26 pagesBenefit-Cost Analysismy.nafi.pmp5283No ratings yet
- Building Information Modeling and Green DesignDocument18 pagesBuilding Information Modeling and Green Designmy.nafi.pmp5283No ratings yet
- Building Information Modeling and Green DesignDocument18 pagesBuilding Information Modeling and Green Designmy.nafi.pmp5283No ratings yet
- Business Case TemplateDocument12 pagesBusiness Case Templatemy.nafi.pmp5283No ratings yet
- Charts and Graphs TemplateDocument5 pagesCharts and Graphs Templatemy.nafi.pmp5283No ratings yet
- النسبيةDocument222 pagesالنسبيةAhmedUp100% (3)
- Solution:: Example Calculate Compound Interest Earned On Rs. 750 Invested at 12% Per Annum For 8 YearsDocument2 pagesSolution:: Example Calculate Compound Interest Earned On Rs. 750 Invested at 12% Per Annum For 8 Yearsmy.nafi.pmp5283No ratings yet
- WP Content Uploads 2018 06 Project Manager To Do List TemplateDocument1 pageWP Content Uploads 2018 06 Project Manager To Do List Templatemy.nafi.pmp5283No ratings yet
- Balloon Loan Calculator: InputsDocument9 pagesBalloon Loan Calculator: Inputsmy.nafi.pmp5283No ratings yet
- Comparison of MethodsDocument3 pagesComparison of MethodsamizahdNo ratings yet
- Gantt Chart LDocument8 pagesGantt Chart LAshok PuttaparthyNo ratings yet
- What Does BIM Mean For Civil EngineersDocument6 pagesWhat Does BIM Mean For Civil Engineersmy.nafi.pmp5283No ratings yet
- Method Key Ratio AnalysisDocument4 pagesMethod Key Ratio Analysismy.nafi.pmp5283No ratings yet
- Asphalt PASERManualDocument32 pagesAsphalt PASERManualSuhaidi AliasNo ratings yet
- Microsoft Excel Sheet For Calculating (Money) Future & Present Value, Amortization Table, Present Value, Power of Compounding, EMI Calculation, MortgageDocument7 pagesMicrosoft Excel Sheet For Calculating (Money) Future & Present Value, Amortization Table, Present Value, Power of Compounding, EMI Calculation, MortgageVikas Acharya100% (1)
- SIPOC AdaptiveBMSDocument9 pagesSIPOC AdaptiveBMSmy.nafi.pmp5283No ratings yet
- Bus Case TempDocument15 pagesBus Case TempAbdul wadoodNo ratings yet
- Guide PEST Analysis GuideDocument5 pagesGuide PEST Analysis Guidemy.nafi.pmp5283No ratings yet
- Pre-Test: A. Clear, Concise, Complete, Correct B. Correct, Crisp, Complete, Confident C. Careful, Calm, Clear, CollectedDocument1 pagePre-Test: A. Clear, Concise, Complete, Correct B. Correct, Crisp, Complete, Confident C. Careful, Calm, Clear, Collectedmy.nafi.pmp5283No ratings yet
- Method Pareto Method 80 20Document5 pagesMethod Pareto Method 80 20my.nafi.pmp5283No ratings yet
- Personal Action PlanDocument1 pagePersonal Action Planmy.nafi.pmp5283No ratings yet
- Method SWOT AnalysisDocument3 pagesMethod SWOT Analysismy.nafi.pmp5283No ratings yet
- Bus Case TempDocument15 pagesBus Case TempAbdul wadoodNo ratings yet
- Gail Carlson, MPH PH.D, State Health Education Specialist, University of Missouri ExtensionDocument9 pagesGail Carlson, MPH PH.D, State Health Education Specialist, University of Missouri ExtensionRahmat ShahNo ratings yet
- Intradermal Meds ChecklistDocument2 pagesIntradermal Meds ChecklistMonika Sarmiento100% (1)
- BG - bm.GG.2018. Atención Primaria Del Adulto MayorDocument235 pagesBG - bm.GG.2018. Atención Primaria Del Adulto MayorAlejandro Guzman100% (1)
- EMTALA Ensures Emergency Care Regardless of StatusDocument3 pagesEMTALA Ensures Emergency Care Regardless of StatusVee MendNo ratings yet
- 21st Century Cures Act LetterDocument2 pages21st Century Cures Act LetterPeter SullivanNo ratings yet
- CINI NewsletterDocument6 pagesCINI NewsletterChild in Need InstituteNo ratings yet
- Journal of DiabetesDocument8 pagesJournal of DiabetesMuhammad FajarNo ratings yet
- Prodedural Coding CPT and HCPCSDocument38 pagesProdedural Coding CPT and HCPCSdonna8compton8harmon83% (6)
- Free PDF Pharmaceutical Experimental Design and Interpretation N A Armstrong and K C JamesDocument2 pagesFree PDF Pharmaceutical Experimental Design and Interpretation N A Armstrong and K C JamesBrentNo ratings yet
- Omnicell Cerner Alliance Brochure enDocument2 pagesOmnicell Cerner Alliance Brochure enRonnie EncarnacionNo ratings yet
- Drug Assessment Paper: InstructionsDocument6 pagesDrug Assessment Paper: InstructionsRAZEN PARAS0% (1)
- Maternity Record Keeping 4.0Document24 pagesMaternity Record Keeping 4.0ItaNo ratings yet
- Western Pennsylvania Guide To Good Health - Winter 2013Document52 pagesWestern Pennsylvania Guide To Good Health - Winter 2013GuideToGoodHealthNo ratings yet
- Beatriz Echeverri ResumeDocument1 pageBeatriz Echeverri Resumeapi-436063355No ratings yet
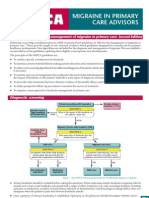
- National Guidelines - MigraineDocument4 pagesNational Guidelines - MigraineSean CardozoNo ratings yet
- Medicare NotesDocument10 pagesMedicare NotesJazmine Royall0% (1)
- Summative Reflection FinalDocument8 pagesSummative Reflection Finalapi-432057546No ratings yet
- CER56 PKU FinalReportDocument343 pagesCER56 PKU FinalReportMonyet...No ratings yet
- HTM ListDocument3 pagesHTM Listamuzik01No ratings yet
- Staying Active for Better HealthDocument1 pageStaying Active for Better HealthAntonia AntoNo ratings yet
- 5S Pocket GuideDocument28 pages5S Pocket Guidesathyabalaraman100% (3)
- Persuasive Speech On HealthcareDocument4 pagesPersuasive Speech On HealthcareRobanderson126No ratings yet
- Dialzyer Reprocessing For Non-Reprocessing StaffDocument31 pagesDialzyer Reprocessing For Non-Reprocessing StaffSitti Zhainab100% (1)
- Medicare Part B Premium Fact SheetDocument2 pagesMedicare Part B Premium Fact SheetTerry PetersonNo ratings yet
- Main Sept 02Document57 pagesMain Sept 02Lindsey RobbinsNo ratings yet
- IELTS Reading - True, False, Not GivenDocument8 pagesIELTS Reading - True, False, Not GivenMiniNo ratings yet
- 2018-08-20 - OR4AD Comment To Task Force - Prices Paid by Oregonians - Rev2Document103 pages2018-08-20 - OR4AD Comment To Task Force - Prices Paid by Oregonians - Rev2Oregonians for Affordable Drug Prices NowNo ratings yet
- MMG ScriptDocument3 pagesMMG ScriptJimmy PinoNo ratings yet
- Healthcare Data Files Just Saved Me AggravationDocument3 pagesHealthcare Data Files Just Saved Me Aggravationpriya_psalmsNo ratings yet
- DDC SVC BRO 0115 Fault CodesDocument16 pagesDDC SVC BRO 0115 Fault CodesAdhem El SayedNo ratings yet