You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Kawasaki DiseaseDocument41 pagesKawasaki DiseaseWuryan Dewi Mftahtyas ArumNo ratings yet
- Pediatric SmleDocument59 pagesPediatric SmleMoayad Zeyad M100% (1)
- Viral and Bacterial Infections of The SkinDocument200 pagesViral and Bacterial Infections of The SkinKarla Jane100% (1)
- Intrauterine InfectionDocument64 pagesIntrauterine Infectionthapan87100% (1)
- Microbial Quality and Safety of Cooked Foods Sold in Urban Schools in Ghana: A Review of Food Handling and Health Implications Ghana A Review of Food Handling and Health ImplicationsDocument10 pagesMicrobial Quality and Safety of Cooked Foods Sold in Urban Schools in Ghana: A Review of Food Handling and Health Implications Ghana A Review of Food Handling and Health ImplicationsresearchpublichealthNo ratings yet
- Groundwater Quality of Boreholes Located Around Cassava Processing MillsDocument7 pagesGroundwater Quality of Boreholes Located Around Cassava Processing MillsresearchpublichealthNo ratings yet
- Screening For Hypertension in The Selected Rural Areas of Tirunelveli District and A Study On Their Lifestyle Related Risk FactorsDocument10 pagesScreening For Hypertension in The Selected Rural Areas of Tirunelveli District and A Study On Their Lifestyle Related Risk FactorsresearchpublichealthNo ratings yet
- Medicine and The Epidemiological Transition To Public HealthDocument7 pagesMedicine and The Epidemiological Transition To Public HealthresearchpublichealthNo ratings yet
- Affordability of Healthcare Services in The Central Gonja District of GhanaDocument12 pagesAffordability of Healthcare Services in The Central Gonja District of GhanaresearchpublichealthNo ratings yet
- Waterborne Diseases Transmission Potential of Sachet Waters Sold in Owerri, Eastern NigeriaDocument6 pagesWaterborne Diseases Transmission Potential of Sachet Waters Sold in Owerri, Eastern NigeriaresearchpublichealthNo ratings yet
- Comparative Analysis of Microbiological and Heavy Metal Characteristics of Tap and Borehole Water in Owerri, Imo State, NigeriaDocument9 pagesComparative Analysis of Microbiological and Heavy Metal Characteristics of Tap and Borehole Water in Owerri, Imo State, NigeriaresearchpublichealthNo ratings yet
- A Trends Analysis of Medical Male Circumcision For HIV Prevention in Eastern and Southern AfricaDocument10 pagesA Trends Analysis of Medical Male Circumcision For HIV Prevention in Eastern and Southern AfricaresearchpublichealthNo ratings yet
- Daily Water Usage and Childhood Diarrheal Morbidity A Case Study of Under - Five in Ahiazu MbaiseDocument7 pagesDaily Water Usage and Childhood Diarrheal Morbidity A Case Study of Under - Five in Ahiazu MbaiseresearchpublichealthNo ratings yet
- Cohort Study Hansana PDFDocument28 pagesCohort Study Hansana PDFTukai KulkarniNo ratings yet
- Vaccination of Healthcare WorkersDocument16 pagesVaccination of Healthcare WorkersBenjamin RuotiNo ratings yet
- Script EFN Hiv AidsDocument3 pagesScript EFN Hiv AidsRina Mulyasari Mar Atussa'adahNo ratings yet
- Communicable Diseases GR.8 HealthDocument40 pagesCommunicable Diseases GR.8 HealthAiza May RosasNo ratings yet
- Performance Task in Empowerment Technologies (Arthur King v. Leaño III, 11-Ipil (ABM-MODULAR)Document13 pagesPerformance Task in Empowerment Technologies (Arthur King v. Leaño III, 11-Ipil (ABM-MODULAR)Mary AuxileNo ratings yet
- Snake Bite First AidDocument6 pagesSnake Bite First Aidmelchor bangaoilNo ratings yet
- Fir DengueDocument2 pagesFir Denguegunalan gunaNo ratings yet
- Postural Vital SignsDocument3 pagesPostural Vital Signsriffs_ahoyNo ratings yet
- DHIS PHC Facility Monthly Report FormDocument4 pagesDHIS PHC Facility Monthly Report FormUmair SaleemNo ratings yet
- Deterministic Malaria Transmission Model With Acquired ImmunityDocument6 pagesDeterministic Malaria Transmission Model With Acquired ImmunityAchmad Nur AlphiantoNo ratings yet
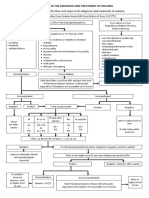
- Algorithm in The Diagnosis and Treatment of MalariaDocument1 pageAlgorithm in The Diagnosis and Treatment of MalariaPearl Monette Cedeño AngNo ratings yet
- Common Beliefs About The Causes of DiseasesDocument7 pagesCommon Beliefs About The Causes of DiseasesSarah Jane GresoNo ratings yet
- Fungal InfectionsDocument8 pagesFungal InfectionskateverdadNo ratings yet
- Gout and Pseudogout PDFDocument3 pagesGout and Pseudogout PDFCarlNo ratings yet
- HerpesDocument3 pagesHerpesNizam UddinNo ratings yet
- WIL - English Does Work 7 Cronica WRITINGDocument2 pagesWIL - English Does Work 7 Cronica WRITINGwilbert edill rodriguez martinez50% (2)
- Low Back Pain in Car Drivers: A Review of Studies Published 1975 To 2005Document15 pagesLow Back Pain in Car Drivers: A Review of Studies Published 1975 To 2005ViolintsarNo ratings yet
- A Review of Electrical Burns Admitted in A Philippine Tertiary Hospital Burn CenterDocument5 pagesA Review of Electrical Burns Admitted in A Philippine Tertiary Hospital Burn CenterRiza Paula LabagnoyNo ratings yet
- Anastrozole Beats Tamoxifen for Postmenopausal Breast CancerDocument9 pagesAnastrozole Beats Tamoxifen for Postmenopausal Breast CancerKiên Võ TrungNo ratings yet
- Malignant Struma OvariiDocument4 pagesMalignant Struma Ovariixwahyu 108No ratings yet
- Morning Report: Pulmonology and Respiratory Medicine Medical Faculty of Sebelas Maret University 2021Document30 pagesMorning Report: Pulmonology and Respiratory Medicine Medical Faculty of Sebelas Maret University 2021debby nirmasariNo ratings yet
- Black Hairy TongueDocument2 pagesBlack Hairy TongueFadhlih MuhammadNo ratings yet
- NCM 111 RRL Chapter 2Document5 pagesNCM 111 RRL Chapter 2kyle ibzNo ratings yet
- Consent FormDocument1 pageConsent FormJulius CagampangNo ratings yet
- Maple Syrup Urine Disease Case StudyDocument5 pagesMaple Syrup Urine Disease Case StudyMaria ClaraNo ratings yet
- Complications of CastingDocument12 pagesComplications of CastingDiana Veroshini GengatharanNo ratings yet