Professional Documents
Culture Documents
CHN Notes
Uploaded by
BrianMarBeltran0 ratings0% found this document useful (0 votes)
134 views50 pageschn notes
Original Title
CHN NOTES
Copyright
© © All Rights Reserved
Available Formats
DOCX, PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this Documentchn notes
Copyright:
© All Rights Reserved
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
0 ratings0% found this document useful (0 votes)
134 views50 pagesCHN Notes
Uploaded by
BrianMarBeltranchn notes
Copyright:
© All Rights Reserved
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
You are on page 1of 50
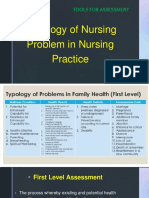
A Typology of Nursing Problems in Family Nursing Practice
First Level Assessment
I. Presence of Wellness Condition-stated as potential or Readiness-a clinical or nursing judgment about a client in
transition from a specific level of wellness or capability to a higher level. Wellness potential is a nursing judgment on
wellness state or condition based on clients performance, current competencies, or performance, clinical data or
explicit expression of desire to achieve a higher level of state or function in a specific area on health promotion and
maintenance. Examples of this are the following
A. Potential for Enhanced Capability for:
1. Healthy lifestyle-e.g. nutrition/diet, exercise/activity
2. Healthy maintenance/health management
3. Parenting
4. Breastfeeding
5. Spiritual well-being-process of clients developing/unfolding of mystery through harmonious interconnectedness that
comes from inner strength/sacred source/God (NANDA 2001)
6. Others. Specify.
B. Readiness for Enhanced Capability for:
1. Healthy lifestyle
2. Health maintenance/health management
3. Parenting
4. Breastfeeding
5. Spiritual well-being
6. Others. Specify.
II. Presence of Health Threats-conditions that are conducive to disease and accident, or may result to failure to
maintain wellness or realize health potential. Examples of this are the following:
A. Presence of risk factors of specific diseases (e.g. lifestyle diseases, metabolic syndrome)
B. Threat of cross infection from communicable disease case
C. Family size beyond what family resources can adequately provide
D. Accident hazards specify.
1. Broken chairs
2. Pointed /sharp objects, poisons and medicines improperly kept
3. Fire hazards
4. Fall hazards
5. Others specify.
E. Faulty/unhealthful nutritional/eating habits or feeding techniques/practices. Specify.
1. Inadequate food intake both in quality and quantity
2. Excessive intake of certain nutrients
3. Faulty eating habits
4. Ineffective breastfeeding
5. Faulty feeding techniques
F. Stress Provoking Factors. Specify.
1. Strained marital relationship
2. Strained parent-sibling relationship
3. Interpersonal conflicts between family members
4. Care-giving burden
G. Poor Home/Environmental Condition/Sanitation. Specify.
1. Inadequate living space
2. Lack of food storage facilities
3. Polluted water supply
4. Presence of breeding or resting sights of vectors of diseases
5. Improper garbage/refuse disposal
6. Unsanitary waste disposal
7. Improper drainage system
8. Poor lightning and ventilation
9. Noise pollution
10. Air pollution
H. Unsanitary Food Handling and Preparation
I. Unhealthy Lifestyle and Personal Habits/Practices. Specify.
1. Alcohol drinking
2. Cigarette/tobacco smoking
3. Walking barefooted or inadequate footwear
4. Eating raw meat or fish
5. Poor personal hygiene
6. Self medication/substance abuse
7. Sexual promiscuity
8. Engaging in dangerous sports
9. Inadequate rest or sleep
10. Lack of /inadequate exercise/physical activity
11. Lack of/relaxation activities
12. Non use of self-protection measures (e.g. non use of bed nets in malaria and filariasis endemic areas).
J. Inherent Personal Characteristics-e.g. poor impulse control
K. Health History, which may Participate/Induce the Occurrence of Health Deficit, e.g. previous history of difficult
labor.
L. Inappropriate Role Assumption- e.g. child assuming mothers role, father not assuming his role.
M. Lack of Immunization/Inadequate Immunization Status Specially of Children
N. Family Disunity-e.g.
1. Self-oriented behavior of member(s)
2. Unresolved conflicts of member(s)
3. Intolerable disagreement
O. Others. Specify._________
III. Presence of health deficits-instances of failure in health maintenance.
Examples include:
A. Illness states, regardless of whether it is diagnosed or undiagnosed by medical practitioner.
B. Failure to thrive/develop according to normal rate
C. Disability-whether congenital or arising from illness; transient/temporary (e.g. aphasia or temporary paralysis
after a CVA) or permanent (e.g. leg amputation secondary to diabetes, blindness from measles, lameness from polio)
IV. Presence of stress points/foreseeable crisis situations-anticipated periods of unusual demand on the
individual or family in terms of adjustment/family resources. Examples of this include:
A. Marriage
B. Pregnancy, labor, puerperium
C. Parenthood
D. Additional member-e.g. newborn, lodger
E. Abortion
F. Entrance at school
G. Adolescence
H. Divorce or separation
I. Menopause
J. Loss of job
K. Hospitalization of a family member
L. Death of a member
M. Resettlement in a new community
N. Illegitimacy
O. Others, specify.___________
Second-Level Assessment
I. Inability to recognize the presence of the condition or problem due to:
A. Lack of or inadequate knowledge
B. Denial about its existence or severity as a result of fear of consequences of diagnosis of problem, specifically:
1. Social-stigma, loss of respect of peer/significant others
2. Economic/cost implications
3. Physical consequences
4. Emotional/psychological issues/concerns
C. Attitude/Philosophy in life, which hinders recognition/acceptance of a problem
D. Others. Specify _________
II. Inability to make decisions with respect to taking appropriate health action due to:
A. Failure to comprehend the nature/magnitude of the problem/condition
B. Low salience of the problem/condition
C. Feeling of confusion, helplessness and/or resignation brought about by perceive magnitude/severity of the
situation or problem, i.e. failure to breakdown problems into manageable units of attack.
D. Lack of/inadequate knowledge/insight as to alternative courses of action open to them
E. Inability to decide which action to take from among a list of alternatives
F. Conflicting opinions among family members/significant others regarding action to take.
G. Lack of/inadequate knowledge of community resources for care
H. Fear of consequences of action, specifically:
1. Social consequences
2. Economic consequences
3. Physical consequences
4. Emotional/psychological consequences
I. Negative attitude towards the health condition or problem-by negative attitude is meant one that interferes with
rational decision-making.
J. In accessibility of appropriate resources for care, specifically:
1. Physical Inaccessibility
2. Costs constraints or economic/financial inaccessibility
K. Lack of trust/confidence in the health personnel/agency
L. Misconceptions or erroneous information about proposed course(s) of action
M. Others specify._________
III. Inability to provide adequate nursing care to the sick, disabled, dependent or vulnerable/
at risk member of the family due to:
A. Lack of/inadequate knowledge about the disease/health condition (nature, severity, complications, prognosis
and management)
B. Lack of/inadequate knowledge about child development and care
C. Lack of/inadequate knowledge of the nature or extent of nursing care needed
D. Lack of the necessary facilities, equipment and supplies of care
E. Lack of/inadequate knowledge or skill in carrying out the necessary intervention or treatment/
procedure of care (i.e. complex therapeutic regimen or healthy lifestyle program).
F. Inadequate family resources of care specifically:
1. Absence of responsible member
2. Financial constraints
3. Limitation of luck/lack of physical resources
G. Significant persons unexpressed feelings (e.g. hostility/anger, guilt, fear/anxiety, despair, rejection) which his/
her capacities to provide care.
H. Philosophy in life which negates/hinder caring for the sick, disabled, dependent, vulnerable/at risk member
I. Members preoccupation with on concerns/interests
J. Prolonged disease or disabilities, which exhaust supportive capacity of family members.
K. Altered role performance, specify.
1. Role denials or ambivalence
2. Role strain
3. Role dissatisfaction
4. Role conflict
5. Role confusion
6. Role overload
L. Others. Specify._________
IV. Inability to provide a home environment conducive to health maintenance and personal development due to:
A. Inadequate family resources specifically:
1. Financial constraints/limited financial resources
2. Limited physical resources-e.i. lack of space to construct facility
B. Failure to see benefits (specifically long term ones) of investments in home environment improvement
C. Lack of/inadequate knowledge of importance of hygiene and sanitation
D. Lack of/inadequate knowledge of preventive measures
E. Lack of skill in carrying out measures to improve home environment
F. Ineffective communication pattern within the family
G. Lack of supportive relationship among family members
H. Negative attitudes/philosophy in life which is not conducive to health maintenance and personal development
I. Lack of/inadequate competencies in relating to each other for mutual growth and maturation
(e.g. reduced ability to meet the physical and psychological needs of other members as a result of familys
preoccupation with current problem or condition.
J. Others specify._________
V. Failure to utilize community resources for health care due to:
A. Lack of/inadequate knowledge of community resources for health care
B. Failure to perceive the benefits of health care/services
C. Lack of trust/confidence in the agency/personnel
D. Previous unpleasant experience with health worker
E. Fear of consequences of action (preventive, diagnostic, therapeutic, rehabilitative) specifically :
1. Physical/psychological consequences
2. Financial consequences
3. Social consequences
F. Unavailability of required care/services
G. Inaccessibility of required services due to:
1. Cost constrains
2. Physical inaccessibility
H. Lack of or inadequate family resources, specifically
1. Manpower resources, e.g. baby sitter
2. Financial resources, cost of medicines prescribe
I. Feeling of alienation to/lack of support from the community, e.g. stigma due to mental illness, AIDS, etc.
J. Negative attitude/ philosophy in life which hinders effective/maximum utilization of community resources for
health care
K. Others, specify __________
Communicable Disease (Vector Borne)
Leptospirosis (Weils disease)
An infectious disease that affects humans and animals, is considered the most common zoonosis in the world
Causative Agent: Leptospira interrogans
Sign/Symptoms:
High fever
Chills
Vomiting
Red eyes
Diarrhea
Severe headache
muscle aches
may include jaundice (yellow skin and eyes)
abdominal pain
Treatment:
PET - > Penicillins, Erythromycin, Tetracycline
Malaria
Malaria (from Medieval Italian: mala aria - "bad air"; formerly called ague or marsh fever) is an infectious
disease that is widespread in many tropical and subtropical regions.
Causative Agent: Anopheles female mosquito
Signs & Symptoms:
Chills to convulsion
Hepatomegaly
Anemia
Sweats profusely
Elevated temperature
Treatment:
Chemoprophylaxis chloroquine taken at weekly interval, starting from 1-2 weeks before entering the endemic area.
Anti-malarial drugs sulfadoxine, quinine sulfate, tetracycline, quinidine
Insecticide treatment of mosquito nets, house spraying, stream seeding and clearing, sustainable preventive
and vector control measles
Preventive Measures: (CLEAN)
Chemically treated mosquito nets
Larvae eating fish
Environmental clean up
Anti mosquito soap/lotion
Neem trees/eucalyptus tree
Filariasis
name for a group of tropical diseases caused by various thread-like parasitic round worms (nematodes)
and their larvae
larvae transmit the disease to humans through a mosquito bite
can progress to include gross enlargement of the limbs and genitalia in a condition called elephantiasis
Sign/Symptoms:
Asymptomatic Stage
Characterized by the presence of microfilariae in the peripheral blood
No clinical signs and symptoms of the disease
Some remain asymptomatic for years and in some instances for life
Acute Stage
Lymphadenitis (inflammation of lymph nodes)
Lymphangitis (inflammation of lymph vessels)
In some cases the male genitalia is affected leading to orchitis (redness, painful and tender scrotum)
Chronic Stage
Hydrocoele (swelling of the scrotum)
Lyphedema (temporary swelling of the upper and lower extremities
Elephantiasis (enlargement and thickening of the skin of the lower and / or upper extremities, scrotum, breast)
Management:
Diethylcarbamazine citrate or Hetrazan
Ivermectin,
Albendazolethe
No treatment can reverse elephantiasis
Schistosomiasis
parasitic disease caused by a larvae
Causative Agent: Schistosoma intercalatum, Schistosoma japonicum, Schistosoma mansoni
Signs & Symptoms: (BALLIPS)
Bulging abdomen
Abdominal pain
Loose bowel movement
Low grade fever
Inflammation of liver & spleen
Pallor
Seizure
Preventive measures
health education regarding mode of transmission and methods of protection; proper disposal of feces and urine;
improvement of irrigation and agriculture practices
Control of patient, contacts and the immediate environment
Treatment:
Diethylcarbamazepine citrate (DEC) or Praziquantel (drug of choice)
Dengue
DENGUE is a mosquito-borne infection which in recent years has become a major international public health concern
It is found in tropical and sub-tropical regions around the world, predominantly in urban and semi-urban areas.
Sign/Symptoms: (VLINOSPARD)
Vomiting
Low platelet
Nausea
Onset of fever
Severe headache
Pain of the muscle and joint
Abdominal pain
Rashes
Diarrhea
Treatment:
The mainstay of treatment is supportive therapy.
o Intravenous fluids
o A platelet transfusion
Reference:
Ms Ma. Adelaida Morong, Far Eastern University- Institute of Nursing
In-House Nursing Review
Communicable Diseases (Chronic)
Chronic
1. Tuberculosis
TB is a highly infectious chronic disease that usually affects the lungs.
Causative Agent: Mycobacterium Tuberculosis
Sign/Symptoms:
cough
afternoon fever
weight loss
night sweat
blood stain sputum
Prevalence/Incidence:
ranks sixth in the leading causes of morbidity (with 114,221 cases) in the Philippines
Sixth leading cause of mortality (with 28507 cases) in the Philippines.
Nursing and Medical Management
Ventilation systems
Ultraviolet lighting
Vaccines, such as the bacillus Calmette Guerin (BCG) vaccine
drug therapy
Preventing Tuberculosis
BCG vaccination
Adequate rest
Balanced diet
Fresh air
Adequate exercise
Good personal Hygiene
National Tuberculosis Control Program key policies
Case finding direct Sputum Microscopy and X-ray examination of TB symptomatics who are negative after 2
or more sputum exams
Treatment shall be given free and on an ambulatory basis, except those with acute complications and emergencies
Direct Observed Treatment Short Course comprehensive strategy to detect and cure TB patients.
DOTS (Direct Observed Treatment Short Course)
Category 1- new TB patients whose sputum is positive; seriously ill patients with severe forms
of smear-negative PTB with extensive parenchymal involvement (moderately- or far advanced) and
extra-pulmonary TB (meningitis, pleurisy, etc.)
o Intensive Phase (given daily for the first 2 months) - Rifampicin + Isioniazid + pyrazinamide + ethambutol.
o If sputum result becomes negative after 2 months, maintenance phase starts. But if sputum is still positive in 2 months
o all drugs are discontinued from 2-3 days and a sputum specimen is examined for culture and drug sensitivity.
The patient resumes taking the 4 drugs for another month and then another smear exam is
done at the end of the 3rd month.
o Maintenance Phase (after 3rd month, regardless of the result of the sputum exam)-INH + rifampicin daily
Category 2-previously-treated patients with relapses or failures.
o Intensive Phase (daily for 3 months, month 1, 2 & 3)-Isioniazid+ rifampicin+ pyrazinamide+ ethambutol+ streptomycin
for the first 2 months Streptomycin+ rifampicin pyrazinamide+ ethambutol on the 3rd month. If sputum is still positive
after 3 months, the intensive phase is continued for 1 more month and then another sputum exam is done.
If still positive after 4 months, intensive phase is continued for the next 5 months.
o Maintenance Phase (daily for 5 months, month 4, 5, 6, 7,& 8)-Isionazid+ rifampicin+ ethambutol
Category 3 new TB patients whose sputum is smear negative for 3 times and chest x-ray result of PTB minimal
o Intensive Phase (daily for 2 months) Isioniazid + rifampicin + pyrazinamide
o Maintenance Phase (daily for the next 2 months) - Isioniazid + rifampicin
2. Leprosy
Sometimes known as Hansen's disease
is an infectious disease caused by , an aerobic, acid fast, rod-shaped mycobacterium
Gerhard Armauer Hansen
Historically, leprosy was an incurable and disfiguring disease
Today, leprosy is easily curable by multi-drug antibiotic therapy
Signs & Symptoms
Early stage (CLUMP) Late Stage (GMISC)
Change in skin color Gynocomastia
Loss in sensation Madarosis(loss of eyebrows)
Ulcers that do not heal Inability to close eyelids (Lagopthalmos)
Muscle weakness Sinking nosebridge
Painful nerves Clawing/contractures of fingers & nose
Prevalence Rate
Metro Manila, the prevalence rate ranged from 0.40 3.01 per one thousand population.
Management:
Dapsone, Lamprene
clofazimine and rifampin
Multi-Drug-Therapy (MDT)
six month course of tablets for the milder form of leprosy and two years for the more severe form
Leprosy Control Program
WHO Classification basis of multi-drug therapy
o Paucibacillary/PB non-infectious types. 6-9 months of treatment.
o Multibacillary/MB infectious types. 24-30 months of treatment.
Multi-drug therapy use of 2 or more drugs renders patients non-infectious a week after starting treatment
o Patients w/ single skin lesion and a negative slit skin smear are treated w/ a single dose of ROM regimen
o For PB leprosy cases- Rifampicin+Dapsone on Day 1 then Dapsone from Day 2-28. 6 blister packs taken monthly within
a max. period of 9 mos.
All patients who have complied w/ MDT are considered cured and no longer regarded as a case of leprosy, even if some
sequelae of leprosy remain.
Responsibilities of the nurse:
o Prevention health education, healthful living through proper nutrition, adequate rest,
sleep and good personal hygiene;
o Casefinding
o Management and treatment prevention of secondary injuries, handling of utensils; special shoes w/ padded soles;
importance of sustained therapy, correct dosage, effects of drugs and the need for medical check-up from
time to time; mental & emotional support
o Rehabilitation-makes patients capable, active and self-respecting member of society.
Reference:
Ms Ma. Adelaida Morong, Far Eastern University- Institute of Nursing
In-House Nursing Review
Community Organizing Participatory Action Research (COPAR)
Definitions of COPAR
A social development approach that aims to transform the apathetic, individualistic and voiceless poor into dynamic,
participatory and politically responsive community.
A collective, participatory, transformative, liberative, sustained and systematic process of building
peoples organizations by mobilizing and enhancing the capabilities and resources of the people for the resolution
of their issues and concerns towards effecting change in their existing oppressive and exploitative conditions
(1994 National Rural Conference)
A process by which a community identifies its needs and objectives, develops confidence to take action in respect
to them and in doing so, extends and develops cooperative and collaborative attitudes and practices in the community
(Ross 1967)
A continuous and sustained process of educating the people to understand and develop their critical awareness
of their existing condition, working with the people collectively and efficiently on their immediate
and long-term problems, and mobilizing the people to develop their capability and readiness to respond and
take action on their immediate needs towards solving their long-term problems (CO: A manual of experience, PCPD)
Importance of COPAR
1. COPAR is an important tool for community development and people empowerment as this helps the
community workers to generate community participation in development activities.
2. COPAR prepares people/clients to eventually take over the management of a development programs in the future.
3. COPAR maximizes community participation and involvement; community resources are mobilized for
community services.
Principles of COPAR
1. People, especially the most oppressed, exploited and deprived sectors are open to change, have the capacity
to change and are able to bring about change.
2. COPAR should be based on the interest of the poorest sectors of society
3. COPAR should lead to a self-reliant community and society.
COPAR Process
A progressive cycle of action-reflection action which begins with small, local and concrete issues identified
by the people and the evaluation and the reflection of and on the action taken by them.
Consciousness through experimental learning central to the COPAR process because it places emphasis on learning
that emerges from concrete action and which enriches succeeding action.
COPAR is participatory and mass-based because it is primarily directed towards and biased in favor of the poor,
the powerless and oppressed.
COPAR is group-centered and not leader-oriented. Leaders are identified, emerge and are tested through action
rather than appointed or selected by some external force or entity.
COPAR Phases of Process
1. Pre-entry Phase
Is the initial phase of the organizing process where the community/organizer looks for communities to serve/help.
It is considered the simplest phase in terms of actual outputs, activities and strategies and time spent for it
Activities include:
o Designing a plan for community development including all its activities and strategies for care development.
o Designing criteria for the selection of site
o Actually selecting the site for community care
2. Entry Phase
Sometimes called the social preparation phase as to the activities done here includes the sensitization of the people
on the critical events in their life, innovating them to share their dreams and ideas on how to manage their concerns
and eventually mobilizing them to take collective action on these.
This phase signals the actual entry of the community worker/organizer into the community. She must be
guided by the following guidelines however.
o Recognizes the role of local authorities by paying them visits to inform them of their presence and activities.
o The appearance, speech, behavior and lifestyle should be in keeping with those of the community residents without
disregard of their being role models.
o Avoid raising the consciousness of the community residents; adopt a low-key profile.
3. Organization Building Phase
Entails the formation of more formal structures and the inclusion of more formal procedures of planning,
implementation, and evaluating community-wide activities. It is at this phase where the organized leaders or
groups are being given trainings (formal, informal, OJT) to develop their skills and in managing their own concerns/
programs.
4. Sustenance and Strengthening Phase
Occurs when the community organization has already been established and the community members
are already actively participating in community-wide undertakings. At this point, the different communities setup in
the organization building phase are already expected to be functioning by way of planning, implementing and
evaluating their own programs with the overall guidance from
the community-wide organization.
Strategies used may include:
o Education and training
o Networking and linkaging
o Conduct of mobilization on health and development concerns
o Implementing of livelihood projects
o Developing secondary leaders
Control of Acute Respiratory Infections (CARI)
Classification
A. No Pneumonia: Cough or Cold
1. No chest in drawing
2. No fast breathing ( <2 mos. - <60/min,2-12 mos. less than 50 per minute; 12 mos. 5 years less than 40 per minute)
Treatment:
1. If coughing more than 30 days, refer for assessment
2. Assess and treat ear problems/sore throat if present
3. Advise mother to give home care
4. Treat fever/wheezing if present
Home Care:
1. Feed the Child
Feed the child during illness
Increase feeding after illness
Clear the nose if it interferes with feeding
2. Increase Fluids
offer the child extra to drink
Increase breastfeeding
3. Soothe the throat and relieve the cough with a safe remedy
4. Watch for the following signs and symptoms and return quickly if they occur
Breathing becomes difficult
Breathing becomes fast
Child is not able to drink
Child becomes sicker
B. Pneumonia
1. No chest in drawing
2. Fast breathing (less than 2 mos- 60/min or more ; 2-12 mos. 50/min or more; 12 mos. 5 years 40/min or more)
Treatment
1. Advise mother to give home care
2. Give an antibiotic
3. Treat fever/wheezing if present
4. If the childs condition gets worst, refer urgently to hospital; if improving, finish 5 days of antibiotic.
Antibiotics Recommended by WHO
Co-trimoxazole,
Amoxycillin, Ampicillin, (p.o)
or Procaine penicillin (I.M.)
C. Severe Pneumonia
1. Chest indrawing
2. Nasal flaring
3. Grunting ( short sounds made with the voice)
4. Cyanosis
Treatment
Refer urgently to hospital
Treat fever ( paracetamol), wheezing ( salbutamol)
D. Very Severe Disease
1. Not able to drink
2. Convulsions
3. Abnormally sleepy or difficult to wake
4. Stridor in calm child
5. Severe undernutrition
Treatment
Refer urgently to hospital
Assessment of Respiratory Infection
Ask the Mother
1. How old is the child?
2. Is the child coughing? For how long?
3. Age less than 2 months: Has the young infant stopped feeding well?
4. Age 2 months up to 5 years: Is the child able to drink?
5. Has the child had fever? For how long?
6. Has the child had convulsions?
Look, Listen
1. Count the breaths in one minute.
Age Fast Breathing
Less than 2
months
60/minute or
more
2 months- 12
months
50/minute or
more
12 months 5
years
40/minute or
more
2. Look for chest in drawing.
3. Look and listen for stridor. Stridor occurs when there is a narrowing of the larynx, trachea or epiglottis
which interferes with air entering the lungs.
4. Look and listen for wheeze. Wheeze is a soft musical noise which shows signs that breathing out (exhale)
is difficult.
5. See if the child is abnormally sleepy or difficult to wake. (Suspect meningitis)
6. Feel for fever or low body temperature.
7. Check for severe under nutrition
Control of Diarrheal Diseases (CDD)
Management of the Patient with Diarrhea
A. No Dehydration
Condition well, alert
Mouth and Tongue moist
Eyes normal
Thirst drinks normally, not thirsty
Tears present
Skin pinch goes back quickly
TREATMENT PLAN A- HOME Treatment.
Three Rules for Home Treatment
1. Give the child more fluids than usual
o use home fluid such as cereal gruel
o give ORESOL, plain water
2. Give the child plenty of food to prevent under nutrition
o continue to breastfeed frequently
o if child is not breastfeed, give usual milk
o if child is less than 6 months and not yet taking solid food, dilute milk for 2 days
o if child is 6 months or older and already taking solid food, give cereal or other starchy food mixed with vegetables,
meat or fish; give fresh fruit juice or mashed banana to provide potassium; feed child at least 6 times a day.
After diarrhea stops, give an extra meal each day for two weeks.
3. Take the child to the health worker if the child does not get better in 3 days or develops any of the following:
o many watery stools
o repeated vomiting
o marked thirst
o eating or drinking poorly
o fever
o blood in the stool
Oresol Treatment
Age Amount of ORS to give
after each loose stool
Amount of ORS to provide
for use at home
< 24
months
50-100 ml 500 ml/day
2-10
years
100- 200 ml 1000 ml/day
10 years
up
As much as wanted 2000 ml/day
B. Some Dehydration
Condition restless, irritable
Mouth and Tongue dry
Eyes sunken
Thirst thirsty, drinks eagerly
Tears absent
Skin pinch goes back slowly
WEIGH PT, TTT. PLAN B
Approximate amount of ORS to give in 1st 4 hours
Age Weight (kg) ORS (ml)
4 months 5 200- 400
4- 11 months 5- 7.9 400- 600
12-23 months 8- 10.9 600- 800
2-4 yrs. 11- 15.9 800-
1200
5-14 yrs. 16- 29.9 1200-
2200
15 yrs. up 30 up 2200-
4000
1. If the child wants more ORS than shown, give more
2. Continue breastfeeding
3. For infants below 6 mos. who are not breastfeed, give 100-200 ml clean water during the period
4. For a child less than 2 years give a teaspoonful every 1-2 min.
5. If the child vomits, wait for 10 min, then continue giving ORS, 1 tbsp/2-3 min
6. If the childs eyelids become puffy, stop ORS, give plain water or breast milk, Resume ORS when puffiness is gone
7. If ( -) signs of DHN- shift to Plan A
Use of Drugs during Diarrhea
Antibiotics should only be used for dysentery and suspected cholera
Antiparasitic drugs should only be used for amoebiasis and giardiasis
C. Severe Dehydration
Condition lethargic or unconscious; floppy
Eyes very sunken and dry
Tears absent
Mouth and tongue very dry
Thirst- drinks poorly or not able to drink
Skin pinch goes back very slowly
Treatment PLAN C- treat quickly
1. Bring pt. to hospital
2. IVF Lactated Ringers Solution or Normal Saline
3. Re-assess pt. Every 1-2 hrs
4. Give ORS as soon as the pt. can drink
Role of Breastfeeding in the Control of Diarrheal Diseases Program
Two problems in CDD
1. High child mortality due to diarrhea
2. High diarrhea incidence among under fives
Highest incidence in age 6 23 months
Highest mortality in the first 2 years of life
Main causes of death in diarrhea :
o Dehydration
To prevent dehydration, give home fluids am as soon as diarrhea starts and if dehydration is present,
rehydrate early, correctly and effectively by giving ORS
o Malnutrition
For under nutrition, continue feeding during diarrhea especially breastfeeding.
Interventions to prevent diarrhea
1. breastfeeding
2. improved weaning practices
3. use of plenty of clean water
4. hand washing
5. use of latrines
6. proper disposal of stools of small children
7. measles immunization
Breastfeeding
1. Risk of severe diarrhea 10-30x higher in bottle fed infants than in breastfed infants.
2. Advantages of breastfeeding in relation to CDD
a. Breast milk is sterile
b. Presence of antibodies protection against diarrhea
c. Intestinal Flora in BF infants prevents growth of diarrhea causing bacteria.
3. Breastfeeding decreases incidence rate by 8-20% and mortality by 24- 27% in infants under 6 months of age.
4. When to wean?
4-6 months soft mashed foods 2x a day
6 months variety of foods 4x a day
Summary of WHO-CDD recommended strategies to prevent diarrhea
1. Improved Nutrition
Exclusive breastfeeding for the first 4-6 months of life and partially for at least one year.
Improved weaning practices
2. Use of safe water
collecting plenty of water from the cleanest source
protecting water from contamination at the source and in the home
3. Good personal and domestic hygiene
handwashing
use of latrines
proper disposal of stools of young children
4. Measles immunization
Department of Health (DOH)
Vision
Health for all Filipinos
Mission
Ensure accessibility & quality of health care to improve the quality of life of all Filipinos, especially the poor.
National Objectives
1. Improve the general health status of the population (reduce infant mortality rate, reduce child morality rate,
2. reduce maternal mortality rate, reduce total fertility rate, increase life expectancy & the quality of life years).
3. Reduce morbidity, mortality, disability & complications from Diarrheas, Pneumonias, Tuberculosis, Dengue,
Intestinal Parasitism, Sexually Transmitted Diseases, Hepatitis B, Accident & Injuries, Dental Caries &
Periodontal Diseases, Cardiovascular Diseases, Cancer, Diabetes, Asthma & Chronic Obstructive Pulmonary Diseases,
Nephritis & Chronic Kidney Diseases, Mental Disorders, Protein Energy Malnutrition, and Iron Deficiency Anemia
& Obesity.
4. Eliminate the ff. diseases as public health problems:
1. Schistosomiasis
2. Malaria
3. Filariasis
4. Leprosy
5. Rabies
6. Measles
7. Tetanus
8. Diphtheria & Pertussis
9. Vitamin A Deficiency & Iodine Deficiency Disorders
5. Eradicate Poliomyelitis
6. Promote healthy lifestyle through healthy diet & nutrition, physical activity & fitness, personal hygiene,
7. mental health & less stressful life & prevent violent & risk-taking behaviors.
8. Promote the health & nutrition of families & special populations through child, adolescent & youth, adult health,
womens health, health of older persons, health of indigenous people, health of migrant workers and
health of different disabled persons and of the rural & urban poor.
9. Promote environmental health and sustainable development through the promotion and maintenance of healthy homes,
schools, workplaces, establishments and communities towns and cities.
Basic Principles to Achieve Improvement in Health
1. Universal access to basic health services must be ensured.
2. The health and nutrition of vulnerable groups must be prioritized.
3. The epidemiological shift from infection to degenerative diseases must be managed.
4. The performance of the health sector must be enhanced.
Primary Strategies to Achieve Goals
1. Increasing investment for Primary Health Care.
2. Development of national standards and objectives for health.
3. Assurance of health care.
4. Support to the local system development.
5. Support for frontline health workers.
Expanded Program for Immunization (EPI)
Principles of EPI
1. Epidemiological situation
2. Mass approach
3. Basic Health Service
The 7 immunizable diseases
1. Tuberculosis
2. Diptheria
3. Pertussis
4. Measles
5. Poliomyelitis
6. Tetanus
7. Hepatitis B
Target Setting
Infants 0-12 months
Pregnant and Post Partum Women
School Entrants/ Grade 1 / 7 years old
Objectives of EPI
To reduce morbidity and mortality rates among infants and children from six childhood immunizable disease
Elements of EPI
Target Setting
Cold chain Logistic Management- Vaccine distribution through cold chain is designed to ensure that the vaccines
were maintained under proper environmental condition until the time of administration.
Information, Education and Communication (IEC)
Assessment and evaluation of Over-all performance of the program
Surveillance and research studies
Administration of vaccines
Vaccine Content Form & Dosage # of
Doses
Route
BCG (Bacillus Calmette
Guerin)
Live attenuated
bacteria
Freeze dried
Infant- 0.05ml
Preschool-0.1ml
1 ID
DPT (Diphtheria
Pertussis Tetanus)
DT- weakened
toxin
P-killed bacteria
liquid-0.5ml 3 IM
OPV (Oral Polio
Vaccine)
weakened virus liquid-2drops 3 Oral
Hepatitis B Plasma derivative Liquid-0.5ml 3 IM
Measles Weakened virus Freeze dried-
0.5ml
1 Subcutaneous
Schedule of Vaccines
Vaccine Age at 1st
dose
Interval
between dose
Protection
BCG At birth BCG is given at the earliest
possible age protects against
the possibility of TB infection
from the other family
members
DPT 6 weeks 4 weeks An early start with DPT
reduces the chance of severe
pertussis
OPV 6weeks 4weeks The extent of protection
against polio is increased the
earlier OPV is given.
Hepa B @ birth @birth,6th
week,14th
week
An early start of Hepatitis B
reduces
the chance of being infected
and becoming a carrier.
Measles 9m0s.-11m0s. At least 85% of measles can
be prevented by immunization
at this age.
6 months earliest dose of measles given in case of outbreak
9months-11months- regular schedule of measles vaccine
15 months- latest dose of measles given
4-5 years old- catch up dose
Fully Immunized Child (FIC)- less than 12 months old child with complete immunizations of DPT, OPV, BCG,
Anti Hepatitis, Anti measles.
Tetanus Toxiod Immunization
Schedule for Women
Vaccine Minimum age
interval
%
protected
Duration
of
Protection
TT1 As early as
possible
0% 0
TT2 4 weeks later 80% 3 years
TT3 6 months later 95% 5 years
TT4 1year
later/during
next pregnancy
99% 10 years
TT5 1 year
later/third
pregnancy
99% Lifetime
There is no contraindication to immunization except when the child is immunosuppressed or is very, very ill
(but not slight fever or cold). Or if the child experienced convulsions after a DPT or measles vaccine,
report such to the doctor immediately.
Malnutrition is not a contraindication for immunizing children rather; it is an indication for immunization
since common childhood diseases are often severe to malnourished children.
Cold Chain under EPI
Cold Chain is a system used to maintain potency of a vaccine from that of manufacture to the time it is given to child
or pregnant woman.
The allowable timeframes for the storage of vaccines at different levels are:
o 6months- Regional Level
o 3months- Provincial Level/District Level
o 1month-main health centers-with ref.
o Not more than 5days- Health centers using transport boxes.
Most sensitive to heat: Freezer (-15 to -25 degrees C)
o OPV
o Measles
Sensitive to heat and freezing (body of ref. +2 to +8 degrees Celsius)
o BCG
o DPT
o Hepa B
o TT
Use those that will expire first, mark X/ exposure, 3rd- discard,
Transport-use cold bags let it stand in room temperature for a while before storing DPT.
Half life packs: 4hours-BCG, DPT, Polio, 8 hours-measles, TT, Hepa B.
FEFO (first expiry and first out) - vaccine is practiced to assure that all vaccines are utilized before
the expiry date. Proper arrangement of vaccines and/or labeling of vaccines expiry date are done to identify
those near to expire vaccines.
DOH Programs
Dental Health Program
To improve the quality of life of the people through the attainment of the highest possible oral health.
Objective: To prevent and control dental diseases and conditions like dental caries and periodontal diseases
thus reducing their prevalence.
Osteoporosis Program
It is characterized by a decrease in bone mass and density that progresses without a symptom or
pain until a fracture occurs generally in the hip, spine or wrist.
Objectives:
o To increase awareness on the prevention and control of osteoporosis as a chronic debilitating condition;
o To increase awareness by physicians and other health professionals on the screening, treatment and
rehabilitation of osteoporosis;
o To empower people with knowledge and skills to adopt healthy lifestyle in preventing the occurrence of osteoporosis.
Health Education & CO
Accepted activity at all levels of public health used as a means of improving the health of the people
through techniques which may influence peoples thought motivation, judgment and action.
Three aspects of health education:
Information
Communication
Education
Sequence of steps in health education:
Creating awareness
Creating motivation
Decision making action
Reproductive Health
1. Family Planning
2. MCH & Nutrition
3. Prevention / treatment of Reproductive Tract Infection & STD
4. Prevention of abortion & its complication
5. Education & counseling on sexuality & sexual health
6. Adolescent sexual reproductive health
7. Violence against women
8. Mens reproductive health (Male sexual disorder )
9. Breast CA & other gyne problem
10. Prevention / treatment of infertility
Older Persons Health Services
Participation in the celebration of Healthy National Elderly Week (Oct 1-7)
o Lecture on healthy lifestyle for the elderly
Provision of drugs for the elderly (20% discount)
Guidelines for Good Nutrition
Nutritional Guidelines are primary recommendations to promote good health through proper nutrition.
Activities:
1. Malnutrition Rehabilitation Program
Targeted Food Task Force Assistance Program (TFAP)
Nutrition Rehabilitation Ward
Akbayan sa Kalusugan sa Kabataan (ASK Project)
2. Micronutrient Supplementation Program
23 in 93
Fortified Vitamin Rice
Health for More in 94
Buwan ng Kabataan, Pag-asa ng Bayan
National Focus: National Micronutrient Day or Araw ng Sangkap Pinoy
Protein Energy Malnutrition
1. Marasmus looks like an old worried man
o Less subcutaneous fats
2. Kwashiorkor - a moon face child
o With flag sign (hair changes)
Vitamin A Deficiency
Respiratory Infection Control
Provision of medicines
Consultative meetings with CARI coordinators
Monitoring of health facilities on the implementation of the program
Alternative Medicine
RA 8423
23 IN 93
Herbal Medicine (LUBBY SANTA)
Herbal Medicine USES
Lagundi ( Vitex Negundo)
SHARED
Skin diseases
Headache,
Asthma,fever,cough&colds
Rheumatism
Eczema
Dysentery
Ulasimang Bato (Peperonia Pellucida) Lowers uric acid
Bawang ( Allium Sativum) HAT Headache and Tootache
Bayabas ( Psidium Guajava) Anti septic, Anti-diarrheal
Yerba Buena (Mentha Cordifolia) Rheumatism and other body aches,
analgesics
Sambong (Blumea Balsamifera) Edema, diuretics
Akapulko Fungal infection, skin diseases
Niog Niogan (Quisqualis Indica) Anti-helminthic
Tsaang Gubat (Carmona Retusa) Diarrhea
Ampalaya (Momordica Charantia) DM
Maternal- Child Care
I. Maternal Care
1. Family Planning
A. Spacing / Artificial Method
a. Hormonal
b. Mechanical & Barrier
c. Biologic
d. Natural
B. Permanent (surgical/irreversible)
a. Tubal Ligation
b. Vasectomy
C. Behavioral Method
2. Breastfeeding
II. Child Care
1. Under Five Care Program
o A package of child health-related services focused to the 0-59 months old children to assure their wellness
and survival
Growth Monitoring Chart (GMC)
o A standard tool used in health centers to record vital information related to child growth and development,
to assess signs of malnutrition.
2. Expanded Program on Immunization
Legal Basis:
PD #996 Compulsory basic
PP #147 National Immunization Day
PP #773 Knock out Polio Days
PP # 1064 polio eradication campaign
PP #4 - Ligtas Tigdas month
Mental Health
A state of well-being where a person can realize his or her own abilities, to cope with the normal stresses of life
and work productively
Components of Mental Health Program
Stress Management and Crisis Intervention
Drugs and Alcohol Abuse Rehabilitation
Treatment and Rehabilitation of Mentally-Ill Patients
Special Project for Vulnerable Groups
Sentrong Sigla Movement
Aim: to promote availability of quality health services
4 pillars:
Quality assurance
Grants & technical assistance
Health promotion
Award
Community Organizing Participatory Action Research
Community Organizing
A continuous and sustained process of;
o EDUCATING THE PEOPLE,
o CRITICAL AWARENESS
o MOBILIZING
Participatory Action Research
A combination of education, research and action.
The purpose is the EMPOWERMENT of people
4 Phases:
Pre entry
Entry
Organizational Building
Sustenance and Strengthening
Laws Affecting CHN Implementation
RA 8749 - Clean Air Act (2000)
RA 6425 Dangerous Drug Act: sale, administration and distribution of prohibited drugs is punishable by law
RA 9173
RA 2382 Philippines Medical Act: define the practice of medicine in the Philippines
RA 1082 Rural Health Act: employment of more physicians, nurses, midwives who will live in the rural areas
to help raise the health condition.
RA 3573 - Reporting of Communicable Disease
RA 6675 Generic Act: promotes, requires and ensures the production of an adequate supply, distribution,
and use of drugs identified by their generic names.
RA 6365
RA 6758
RA 4703
RA 7305 Magna Carta for Public Health Workers (approved by Pres. Corazon C. Aquino): aims to promote
and improve the social and economic well being of health workers, their living and conditions.
RA 7160 Local Government Code: responsibility for the delivery of basic services of the national government
Reference:
Ms Ma. Adelaida Morong, Far Eastern University- Institute of Nursing
In-House Nursing Review
Garantisadong Pambata (GP)
Definition
Garantisadong Pambata is a biannual week long delivery of a package of health services to children between the
ages of 0-59 months old with the purpose of reducing morbidity and mortality among under fives through the
promotion of positive Filipino values for proper child growth and development.
Routine Health Services
Health Service Dosage Route of Administration Target Population
Vitamin A
capsule
200,000 IU
or 1 capsule
100,000 IU or
cap or 3
drops
Orally by drops 12-59 months old,
nationwide
9-12 months old infants
receiving AMV nationwide
Ferrous
Sulfate
(25 mg.
Elemental Iron
per ml; 30 ml.
Bottle as taken
home medicine
with
instructions)
0.3ml(2-6
mos) once a
day
0.6ml(6-
11mos) once a
day
Orally by drops
2-11 months old infants in
Mindanao area, including
evacuation centers in
armed conflict areas.
Routine
Immunization
-BCG*
-DPT*
-OPV*
-AMV*
-Hepa B (if
available)
0.05ml
0.5ml
2 drops
0.5ml
0.5ml
Intradermal on right deltoid
Intramuscularly on anterior
thigh
Orally
Subcutaneously on deltoid
Intramuscularly
Nationwide
0-11 mos
0-11 mos
0-11 mos
9-11 mos
0-11 mos
Deworming
drug
(if available)
1 tablet as
single dose
Orally 36-59 mos, nationwide
Weighing 0-59 mos, nationwide
o The child should not have received megadose of Vit. A above the recommended dosage within the past 4 weeks except
if the child has measles or signs and symptoms of Vit A. deficiency.
o For any child between 12-23 months, who missed any of his routine immunization, the health worker should give
the child the necessary antigen to complete FIC and shall be recorded as such.
Garantisadong Pambata
Sangkap Pinoy
Vitamin A, Iron and Iodine
Sources: green leafy and yellow vegetables, fruits, liver, seafoods, iodized salt, pan de bida and other fortified foods.
These micronutrients are not produced by the body, and must be taken in the food we eat; essential in the normal process of growth and development:
1. Helps the body to regulate itself
2. Necessary in energy metabolism
3. Vital in brain cell formation and mental development
4. Necessary in the body immune system to protect the body from severe infection.
5. Eating Sangkap Pinoy-rich foods can prevent and control:
Protein Energy Malnutrition
Vitamin A Deficiency
Iron Deficiency Anemia
Iodine Deficiency Disorder
Breastfeeding
Breast milk is best for babies up to 2 years old. Exclusive breastfeeding is recommended for the first six months
of life. At about six months, give carefully selected nutritious foods as supplements.
Breastfeeding provides physical and psychological benefits for children and mothers as well as economic benefits
for families and societies.
Benefits:
For infants
1. Provides a nutritional complete food for the young infant.
2. Strengthens the infants immune system, preventing many infections.
3. Safely rehydrates and provides essential nutrients to a sick child, especially to those suffering
from diarrheal diseases.
4. Reduces the infants exposure to infection.
For the Mother
1. Reduces a womans risk of excessive blood loss after birth
2. Provides a natural method of delaying pregnancies.
3. Reduces the risk of ovarian and breast cancers and osteoporosis.
For the Family and Community
1. Conserves funds that otherwise would be spent on breast milk substitute, supplies and fuel to prepare them.
2. Saves medical costs to families and governments by preventing illnesses and by providing immediate postpartum
contraception.
Complimentary Feeding for Babies 6-11 Months Old
What are Complementary Foods?
1. foods introduced to the child at the age 6 months to supplement breastmilk
2. Given progressively until the child is used to three meals and in-between feedings at the age of one year.
Why is there a Need to Give Complementary Foods?
1. breastmilk can be a single source of nourishment from birth up to six months of life.
2. The childs demands for food increases as he grows older and breastmilk alone is not enough to meet his
increased nutritional needs for rapid growth and development
3. Breastmilk should be supplemented with other foods so that the child can get additional nutrients
4. Introduction of complementary foods will accustom him to new foods that will also provide additional nutrients
to make him grow well
5. Breastfeeding, however, should continue for as long as the mother is able and has milk which could be as long as
two years
How to Give Complementary Foods for Babies 6-11 Months Old?
1. Prepare mixture of thick lugao/ cooked rice, soft cooked vegetables. Egg yolk, mashed beans, flaked fish/chicken/
ground meat and oil.
2. Give mixture by teaspoons 2-4 times daily, increasing the amount of teaspoons and number of feeding until the
full recommended amount is consumed
3. Give bite-sized fruit separately
4. Give egg alone or combine with above food mixture
Herbal Medicine Plants Approved by the DOH
These are the list of the ten (10) medicinal plants that the Philippine Department of Health (DOH) through its
"Traditional Health Program" has endorsed. All ten (10) herbs have been thoroughly tested and have been clinically
proven to have medicinal value in the relief and treatment of various aliments:
Plant Name:
Uses & Preparation:
Asthma, Cough & Fever - Decoction ( Boil raw fruits or
leaves in 2 glasses of water for 15 minutes)Dysentery,
Colds & Pain - Decoction ( Boil a handful of leaves &
flowers in water to produce a glass, three times a day)
Skin diseases (dermatitis, scabies, ulcer, eczema) -
Wash & clean the skin/wound with the decoction
Headache - Crush leaves may be applied on the forehead
Rheumatism, sprain, contusions, insect bites - Pound
the leaves and apply on affected area
Lagundi (Vitex
negundo)
Plant Name:
Yerba (Hierba )
Buena (Mentha
cordifelia)
Uses & Preparation:
Pain (headache, stomachache) - Boil chopped leaves in 2 glasses
of water for 15 minutes. Divide decoction into 2 parts, drink one
part every 3 hours.
Rheumatism, arthritis and headache - Crush the fresh leaves
and squeeze sap. Massage sap on painful parts with eucalyptus
Cough & Cold - Soak 10 fresh leaves in a glass of hot water,
drink as tea. (expectorant)
Swollen gums - Steep 6 g. of fresh plant in a glass of boiling
water for 30 minutes. Use as a gargle solution
Toothache - Cut fresh plant and squeeze sap. Soak a piece of
cotton in the sap and insert this in aching tooth cavity
Menstrual & gas pain - Soak a handful of leaves in a lass of
boiling water. Drink infusion.
Nausea & Fainting - Crush leaves and apply at nostrils of
patients
Insect bites - Crush leaves and apply juice on affected area or
pound leaves until like a paste, rub on affected area
Pruritis - Boil plant alone or with eucalyptus in water. Use
decoction as a wash on affected area.
Plant Name:
Sambong (Blumea
balsamifera)
Uses & Preparation:
Anti-edema, diuretic, anti-urolithiasis - Boil chopped
leaves in a glass of water for 15 minutes until one glassful
remains. Divide decoction into 3 parts, drink one part 3
times a day.
Diarrhea - Chopped leaves and boil in a glass of water for 15
minutes. Drink one part every 3 hours.
Plant Name:
Tsaang
Gubat (Carmona
retusa)
Uses & Preparation:
Diarrhea - Boil chopped leaves into 2 glasses of water for 15
minutes. Divide decoction into 4 parts. Drink 1 part every 3
hours
Stomachache - Boil chopped leaves in 1 glass of water for 15
minutes. Cool and strain.
Plant Name:
Niyug-
niyogan (Quisqualis
indica L.)
Uses & Preparation:
Anti-helmintic - The seeds are taken 2 hours after supper. If
no worms are expelled, the dose may be repeated after one
week. (Caution: Not to be given to children below 4 years old)
Plant Name:
Bayabas/Guava (Psidium
guajava L.)
Uses & Preparation:
For washing wounds - Maybe use twice a day
Diarrhea - May be taken 3-4 times a day
As gargle and for toothache - Warm decoction is used for
gargle. Freshly pounded leaves are used for toothache. Boil
chopped leaves for 15 minutes at low fire. Do not cover and
then let it cool and strain
Plant Name:
Akapulko (Cassia
alata L.)
Uses & Preparation:
Anti-fungal (tinea flava, ringworm, athletes foot
and scabies) - Fresh, matured leaves are pounded.
Apply soap to the affected area 1-2 times a day
Plant Name:
Ulasimang
Bato(Peperonica
pellucida)
Uses & Preparation:
Lowers uric acid (rheumatism and gout) - One a half cup leaves
are boiled in two glass of water over low fire. Do not cover pot.
Divide into 3 parts and drink one part 3 times a day
Plant Name:
Bawang (Allium
sativum)
Uses & Preparation:
Hypertension - Maybe fried, roasted, soaked in
vinegar for 30 minutes, or blanched in boiled water
for 15 minutes. Take 2 pieces 3 times a day after
meals.
Toothache - Pound a small piece and apply to
affected area
Plant Name
Ampalaya (Mamordica
Charantia)
Uses & Preparation:
Diabetes Mellitus (Mild non-insulin dependent) - Chopped
leaves then boil in a glass of water for 15 minutes. Do not
cover. Cool and strain. Take 1/3 cup 3 times a day after
meals
Reminders on the Use of Herbal Medicine
1. Avoid the use of insecticide as these may leave poison on plants.
2. In the preparation of herbal medicine, use a clay pot and remove cover while boiling at low heat.
3. Use only part of the plant being advocated.
4. Follow accurate dose of suggested preparation.
5. Use only one kind of herbal plant for each type of symptoms or sickness.
6. Stop giving the herbal medication in case untoward reaction such as allergy occurs.
7. If signs and symptoms are not relieved after 2 to 3 doses of herbal medication, consult a doctor.
Sources: Cuevas, Francis Public Health Nursing in the Philippines. 10th Edition 2007
http://www.pcarrd.dost.gov.ph/prosea/proseaherbal
History of Community Health Nursing
Date Event
1901
Act # 157 (Board of Health of the Philippines); Act # 309 (Provincial and Municipal Boards of Health) were created.
1905
Board of Health was abolished; functions were transferred to the Bureau of Health.
1912
Act # 2156 or Fajardo Act created the Sanitary Divisions, the forerunners of present MHOs; male nurses performs
the functions of doctors
1919
Act # 2808 (Nurses Law was created) - Carmen del Rosario, 1st Filipino Nurse supervisor under Bureau of Health
Oct. 22, 1922
Filipino Nurses Organization (Philippine Nurses Organization) was organized.
1923
Zamboanga General Hospital School of Nursing & Baguio General Hospital were established; other government
schools of nursing were organized several years after.
1928
1st Nursing convention was held
1940
Manila Health Department was created.
1941
Dr. Mariano Icasiano became the first city health officer; Office of Nursing was created through the effort of
Vicenta Ponce (chief nurse) and Rosario Ordiz (assistant chief nurse)
Dec. 8, 1941
Victims of World War II were treated by the nurses of Manila.
July 1942
Nursing Office was created; Dr. Eusebio Aguilar helped in the release of 31 Filipino nurses in Bilibid Prison as
prisoners of war by the Japanese.
Feb. 1946
Number of nurses decreased from 556 308.
1948
First training center of the Bureau of Health was organized by the Pasay City Health Department. Trinidad Gomez,
Marcela Gabatin, Costancia Tuazon, Ms. Bugarin, Ms. Ramos, and Zenaida Nisce composed the training staff.
1950
Rural Health Demonstration and Training Center was created.
1953
The first 81 rural health units were organized.
1957
RA 1891 amended some sections of RA 1082 and created the eight categories of rural health unit causing an increase
in the demand for the community health personnel.
1958-1965
Division of Nursing was abolished (RA 977) and Reorganization Act (EO 288)
1961
Annie Sand organized the National League of Nurses of DOH.
1967
Zenaida Nisce became the nursing program supervisor and consultant on the six special diseases
(TB, leprosy, V.D., cancer, filariasis, and mental health illness).
1975
Scope of responsibility of nurses and midwives became wider due to restructuring of the health care delivery system.
1976-1986
The need for Rural Health Practice Program was implemented.
1990- 1992
Local Government Code of 1991 (RA 7160)
1993-1998
Office of Nursing did not materialize in spite of persistent recommendation of the officers, board members,
and advisers of the National League of Nurses Inc.
Jan. 1999
Nelia Hizon was positioned as the nursing adviser at the Office of Public Health Services through
Department Order # 29.
May 24, 1999
EO # 102, which redirects the functions and operations of DOH, was signed by former President Joseph Estrada.
Integrated Management of Childhood Illnesses (IMCI)
Definition
IMCI is an integrated approach to child health that focuses on the well-being of the whole child.
IMCI strategy is the main intervention proposed to achieve a significant reduction in the number of
deaths from communicable diseases in children under five
Goal
By 2010, to reduce the infant and under five mortality rate at least one third, in pursuit of the goal of reducing it
by two thirds by 2015.
Aim
To reduce death, illness and disability, and to promote improved growth and development among children under
5 years of age.
IMCI includes both preventive and curative elements that are implemented by families and communities as well
as by health facilities.
IMCI Objectives
To reduce significantly global mortality and morbidity associated with the major causes of disease in children
To contribute to the healthy growth & development of children
IMCI Components of Strategy
Improving case management skills of health workers
Improving the health systems to deliver IMCI
Improving family and community practices
**For many sick children a single diagnosis may not be apparent or appropriate
Presenting complaint:
Cough and/or fast breathing
Lethargy/Unconsciousness
Measles rash
Very sick young infant
Possible course/ associated condition:
Pneumonia, Severe anemia, P. falciparum malaria
Cerebral malaria, meningitis, severe dehydration
Pneumonia, Diarrhea, Ear infection
Pneumonia, Meningitis, Sepsis
Five Disease Focus of IMCI:
Acute Respiratory Infection
Diarrhea
Fever
Malaria
Measles
Dengue Fever
Ear Infection
Malnutrition
The IMCI Case Management Process
Assess and classify
Identify appropriate treatment
Treat/refer
Counsel
Follow-up
The Integrated Case Management Process
Check for General Danger Signs:
A general danger sign is present if:
o The child is not able to drink or breastfeed
o The child vomits everything
o The child has had convulsions
o The child is lethargic or unconscious
Assess Main Symptoms
Cough/DOB
Diarrhea
Fever
Ear problems
Assess and Classify Cough of Difficulty of Breathing
Respiratory infections can occur in any part of the respiratory tract such as the nose, throat, larynx, trachea,
air passages or lungs.
Assess and classify PNEUMONIA
Cough or difficult breathing
An infection of the lungs
Both bacteria and viruses can cause pneumonia
Children with bacterial pneumonia may die from hypoxia (too little oxygen) or sepsis (generalized infection).
** A child with cough or difficult breathing is assessed for:
How long the child has had cough or difficult breathing
Fast breathing
Chest indrawing
Stridor in a calm child.
Remember:
o ** If the child is 2 months up to 12 months the child has fast breathing if you count 50 breaths per minute or more
o ** If the child is 12 months up to 5 years the child has fast breathing if you count 40 breaths per minute or more.
Color Coding
PINK
(URGENT REFERRAL)
YELLOW
(Treatment at outpatient health facility)
GREEN
(Home management)
OUTPATIENT
HEALTH FACILITY
Pre-referral
treatments
Advise parents
Refer child
OUTPATIENT HEALTH FACILITY
Treat local infection
Give oral drugs
Advise and teach caretaker
Follow-up
HOME
Caretaker is counseled on:
Home treatment/s
Feeding and fluids
When to return
immediately
Follow-up
REFERRAL FACILITY
Emergency Triage and
Treatment ( ETAT)
Diagnosis, Treatment
Monitoring, follow-up
SEVERE PNEUMONIA OR VERY SEVERE
DISEASE
Give first dose of an
appropriate antibiotic
Give Vitamin A
Treat the child to prevent
low blood sugar
Refer urgently to the
hospital
Give paracetamol for fever
> 38.5
o
C
Any general danger
sign or
Chest indrawing or
Stridor in calm child
PNEUMONIA
Give an appropriate
antibiotic for 5 days
Soothe the throat and
relieve cough with a safe
remedy
Advise mother when to
return immediately
Follow up in 2 days
Give Paracetamol for fever
> 38.5
o
C
Fast breathing
NO PNEUMONIA : COUGH OR COLD
If coughing more than
more than 30 days, refer
for assessment
Soothe the throat and
relieve the cough with a
safe remedy
Advise mother when to
return immediately
Follow up in 5 days if not
improving
No signs of pneumonia
or very severe disease
Assess and classify DIARRHEA
A child with diarrhea is assessed for:
How long the child has had diarrhoea
Blood in the stool to determine if the child has dysentery
Signs of dehydration.
Classify DYSENTERY
o Child with diarrhea and blood in the stool
Two of the following signs?
Abnormally sleepy or difficult
to awaken
Sunken eyes
Not able to drink or drinking
poorly
Skin pinch goes back very
slowly
SEVERE
DEHYDRATION
If child has no other severe classification:
o Give fluid for severe dehydration ( Plan C ) OR
If child has another severe classification :
o Refer URGENTLY to hospital with mother giving
frequent sips of ORS on the way
o Advise the mother to continue breastfeeding
If child is 2 years or older and there is cholera in
your area, give antibiotic for cholera
Two of the following signs :
Restless, irritable
Sunken eyes
Drinks eagerly, thirsty
Skin pinch goes back slowly
SOME
DEHYDRATION
Give fluid and food for some dehydration ( Plan B )
If child also has a severe classification :
o Refer URGENTLY to hospital with mother giving
frequent sips of ORS on the way
o Advise mother when to return immediately
Follow up in 5 days if not improving
Not enough signs to classify as
some or severe dehydration
NO
DEHYDRATION
Home Care
Give fluid and food to treat diarrhea at home ( Plan A
)
Advise mother when to return immediately
Follow up in 5 days if not improving
Dehydration present
SEVERE
PERSISTENT
DIARRHEA
Treat dehydration before referral unless the child
has another severe classification
Give Vitamin a
Refer to hospital
No dehydration
PERSISTENT
DIARRHEA
Advise the mother on feeding a child who has
persistent diarrhea
Give Vitamin A
Follow up in 5 days
Blood in the stool
DYSENTERY
Treat for 5 days with an oral antibiotic recommended
for Shigella in your area
Follow up in 2 days
Give also referral treatment
Does the child have fever?
**Decide:
Malaria Risk
No Malaria Risk
Measles
Dengue
Malaria Risk
Any general danger sign or
Stiff neck
VERY SEVERE FEBRILE
DISEASE / MALARIA
Give first dose of quinine ( under
medical supervision or if a hospital is
not accessible within 4hrs )
Give first dose of an appropriate
antibiotic
Treat the child to prevent low blood
sugar
Give one dose of paracetamol in health
center for high fever (38.5
o
C) or above
Send a blood smear with the patient
Refer URGENTLY to hospital
Blood smear ( + )
If blood smear not done:
NO runny nose, and
NO measles, and
NO other causes of fever
MALARIA
Treat the child with an oral
antimalarial
Give one dose of paracetamol in health
center for high fever (38.5
o
C) or above
Advise mother when to return
immediately
Follow up in 2 days if fever persists
If fever is present everyday for more
than 7 days, refer for assessment
Blood smear ( - ), or
Runny nose, or
Measles, or Other causes of
fever
FEVER : MALARIA
UNLIKELY
Give one dose of paracetamol in health
center for high fever (38.5
o
C) or above
Advise mother when to return
immediately
Follow up in 2 days if fever persists
If fever is present everyday for more
than 7 days, refer for assessment
No Malaria Risk
Any general danger sign or
Stiff neck
VERY SEVERE FEBRILE
DISEASE
Give first dose of an appropriate
antibiotic
Treat the child to prevent low blood
sugar
Give one dose of paracetamol in health
center for high fever (38.5
o
C) or above
Refer URGENTLY to hospital
No signs of very severe febrile
disease
FEVER : NO MALARIA
Give one dose of paracetamol in health
center for high fever (38.5
o
C) or above
Advise mother when to return
immediately
Follow up in 2 days if fever persists
If fever is present everyday for more
than 7 days, refer for assessment
Measles
Clouding of cornea or
Deep or extensive mouth ulcers
SEVERE COMPLICATED
MEASLES
Give Vitamin A
Give first dose of an appropriate
antibiotic
If clouding of the cornea or pus
draining from the eye, apply
tetracycline eye ointment
Refer URGENTLY to hospital
Pus draining from the eye or
Mouth ulcers
MEASLES WITH EYE
OR MOUTH
COMPLICATIONS
Give Vitamin A
If pus draining from the eye, apply
tetracycline eye ointment
If mouth ulcers, teach the mother
to treat with gentian violet
Measles now or within the last 3
months
MEASLES
Give Vitamin A
Dengue Fever
Bleeding from nose or gums or
Bleeding in stools or vomitus or
Black stools or vomitus or
Skin petechiae or
Cold clammy extremities or
Capillary refill more than 3
seconds or
Abdominal pain or
Vomiting
Tourniquet test ( + )
SEVERE DENGUE
HEMORRHAGIC
FEVER
If skin petechiae or Tourniquet
test,are the only positive signs give
ORS
If any other signs are positive, give
fluids rapidly as in Plan C
Treat the child to prevent low
blood sugar
DO NOT GIVE ASPIRIN
Refer all children Urgently to
hospital
No signs of severe dengue
hemorrhagic fever
FEVER: DENGUE
HEMORRHAGIC
UNLIKELY
DO NOT GIVE ASPIRIN
Give one dose of paracetamol in
health center for high fever
(38.5
o
C) or above
Follow up in 2 days if fever
persists or child shows signs of
bleeding
Advise mother when to return
immediately
Does the child have an ear problem?
Tender swelling behind the ear
MASTOIDITIS
Give first dose of appropriate
antibiotic
Give paracetamol for pain
Refer URGENTLY
Pus seen draining from the ear and discharge is
reported for less than 14 days or
Ear pain
ACUTE EAR INFECTION
Give antibiotic for 5 days
Give paracetamol for pain
Dry the ear by wicking
Follow up in 5 days
Pus seen draining from the ear and discharge is
reported for less than 14 days
CHRONIC EAR
INFECTION
Dry the ear by wicking
Follow up in 5 days
No ear pain and no pus seen draining from the ear
NO EAR INFECTION
No additional treatment
Check for Malnutrition and Anemia
Give an Appropriate Antibiotic:
A. For Pneumonia, Acute ear infection or Very Severe disease
COTRIMOXAZOLE
BID FOR 5 DAYS
AMOXYCILLIN
BID FOR 5 DAYS
Age or Weight
Adult
tablet
Syrup
Tablet
Syrup
2 months up to 12
months ( 4 - < 9 kg )
1 / 2
5 ml
1 / 2
5 ml
12 months up to 5 years
( 10 19kg )
1
7.5 ml
1
10 ml
B. For Dysentery
COTRIMOXAZOLE
BID FOR 5 DAYS
AMOXYCILLIN
BID FOR 5 DAYS
AGE OR
WEIGHT
TABLET
SYRUP
SYRUP 250MG/5ML
2 4 months
( 4 - < 6kg )
5 ml 1.25 ml ( tsp )
4 12 months
( 6 - < 10 kg )
5 ml 2.5 ml ( tsp )
1 5 years old
( 10 19 kg )
1
7.5 ml ( 1 tsp )
C. For Cholera
TETRACYCLINE
QID FOR 3
DAYS
COTRIMOXAZOLE
BID FOR 3 DAYS
AGE OR WEIGHT Capsule 250mg Tablet Syrup
2 4 months ( 4 - < 6kg ) 1 / 2 5ml
4 12 months ( 6 - < 10 kg ) 1 / 2 5 ml
1 5 years old ( 10 19 kg) 1 1 7.5ml
Give an Oral Antimalarial
CHOLOROQUINE
Give for 3 days
Primaquine
Give single
dose in
health
center for
P.
Falciparum
Primaquine
Give daily
for 14 days
for P. Vivax
Sulfadoxine +
Pyrimethamine
Give single
dose
AGE TABLET ( 150MG ) TABLET
( 15MG)
TABLET
( 15MG)
TABLET
( 15MG)
DAY1 DAY2 DAY3
2months
5months
5 months
12 months
1/2
12months
3 years old
1 1
3 years old -
5 years old
1 1 1 3/4 1/2 1
GIVE VITAMIN A
AGE VITAMIN A
CAPSULES 200,000
IU
6 months 12 months 1/2
12 months 5 years
old
1
GIVE IRON
AGE or WEIGHT Iron/Folate Tablet
FeSo4 200mg + 250mcg
Folate (60mg elemental iron)
Iron Syrup
FeSo4 150 mg/5ml
(6mg elemental iron per ml )
2months-4months
(4 - <6kg )
2.5 ml
4months 12months
(6 - <10kg )
4 ml
12months 3
years (10 - <14kg)
1/2 5 ml
3years 5 years ( 14
19kg )
1/2 7.5 ml
GIVE PARACETAMOL FOR HIGH FEVER (38.5
o
C OR MORE) OR EAR PAIN
AGE OR WEIGHT TABLET ( 500MG ) SYRUP ( 120MG / 5ML )
2 months 3
years ( 4 - <14kg )
5 ml
3 years up to 5
years (14 19 kg )
1/2 10 ml
GIVE MEBENDAZOLE
Give 500mg Mebendazole as a single dose in health center if :
o hookworm / whipworm are a problem in children in your area, and
o the child is 2 years of age or older, and
o the child has not had a dose in the previous 6 months
Reference:
Ms Ma. Adelaida Morong, Far Eastern University- Institute of Nursing
In-House Nursing Review
R.A. 7160 - or the Local Government Code
This involves the devolution of powers, functions and responsibilities to the local government both rural & urban.
The Code aims to transform local government units into self-reliant communities and active partners in the
attainment of national goals thru a more responsive and accountable local government structure instituted thru
a system of decentralization. Hence, each province, city and municipality has a LOCAL HEALTH BOARD (LHB)
which is mandated to propose annual budgetary allocations for the operation and maintenance of their own
health facilities.
Composition of LHB
Provincial Level
1. Governor- chair
2. Provincial Health Officer vice chairman
3. Chairman, Committee on Health of Sangguniang Panlalawigan
4. DOH representative
5. NGO representative
City and Municipal Level
1. Mayor chair
2. MHO vice chair
3. Chairman, Committee on Health of Sangguniang Bayan
4. DOH representative
5. NGO representative
Effective Local Health System Depends on:
1. The LGUs financial capability
2. A dynamic and responsive political leadership
3. Community empowerment
R.A. 2382 Philippine Medical Act.
This act defines the practice of medicine in the country.
R.A. 1082 Rural Health Act.
It created the 1st 81 Rural Health Units.
amended by RA 1891; more physicians, dentists, nurses, midwives and sanitary inspectors will live in the rural
areas where they are assigned in order to raise the health conditions of barrio people ,hence help decrease the
high incidence of preventable diseases
R.A. 6425 Dangerous Drugs Act
It stipulates that the sale, administration, delivery, distribution and transportation of prohibited drugs is
punishable by law.
R.A. 9165 the new Dangerous Drug Act of 2002
P.D. No. 651
Requires that all health workers shall identify and encourage the registration of all births within 30 days
following delivery.
P.D. No. 996
Requires the compulsory immunization of all children below 8 yrs. of age against the 6 childhood immunizable
diseases.
P.D. No. 825
Provides penalty for improper disposal of garbage.
R.A. 8749 Clean Air Act of 2000
P.D. No. 856 Code on Sanitation
It provides for the control of all factors in mans environment that affect health including the quality of water,
food, milk, insects, animal carriers, transmitters of disease, sanitary and recreation facilities, noise, pollution
and control of nuisance.
R.A. 6758
Standardizes the salary of government employees including the nursing personnel.
R.A. 6675 Generics Act of 1988
Which promotes, requires and ensures the production of an adequate supply, distribution, use and acceptance
of drugs and medicines identified by their generic name.
R.A. 6713 Code of Conduct and Ethical Standards of Public Officials and Employees
It is the policy of the state to promote high standards of ethics in public office. Public officials and employees
shall at all times be accountable to the people and shall discharges their duties with utmost responsibility,
integrity, competence and loyalty, act with patriotism and justice, lead modest lives uphold public interest over
personal interest.
R.A. 7305 Magna Carta for Public Health Workers
This act aims: to promote and improve the social and economic well-being of health workers, their living and
working conditions and terms of employment; to develop their skills and capabilities in order that they will be
more responsive and better equipped to deliver health projects and programs; and to encourage those with
proper qualifications and excellent abilities to join and remain in government service.
R.A. 8423
Created the Philippine Institute of Traditional and Alternative Health Care.
P.D. No. 965
Requires applicants for marriage license to receive instructions on family planning and responsible parenthood.
P.D. NO. 79
Defines, objectives, duties and functions of POPCOM
RA 4073
advocates home treatment for leprosy
Letter of Instruction No. 949
legal basis of PHC dated OCT. 19, 1979
promotes development of health programs on the community level
RA 3573
requires reporting of all cases of communicable diseases and administration of prophylaxis
Ministry Circular No. 2 of 1986
includes AIDS as notifiable disease
R.A. 7875 National Health Insurance Act
R.A. 7432 Senior Citizens Act
R. A. 7719 - National Blood Services Act
R.A. 8172 Salt Iodization Act (ASIN LAW)
R.A. 7277- Magna Carta for PWDs \
provides their rehabilitation, self development and self-reliance and integration into
the mainstream of society
A. O. No. 2005-0014- National Policies on Infant and Young Child Feeding:
1. All newborns be breastfeed within 1 hr after birth
2. Infants be exclusively breastfeed for 6 months.
3. Infants be given timely, adequate and safe complementary foods
4. Breastfeeding be continued up to 2 years and beyond
EO 51- Phil. Code of Marketing of Breast milk Substitutes
R.A. - 7600 Rooming In and Breastfeeding Act of 1992
R.A. 8976- Food Fortification Law
R.A. 8980
promulgates a comprehensive policy and a national system for ECCD
A.O. No. 2006- 0015
defines the Implementing guidelines on Hepatitis B Immunization for Infants
R.A. 7846
mandates Compulsory Hepatitis B Immunization among infants and children less than 8 yrs old
R.A. 2029
mandates Liver Cancer and Hepatitis B Awareness Month Act (February)
A.O. No. 2006-0012
specifies the Revised Implementing Rules and Regulations of E.O. 51 or Milk Code, Relevant International
Agreements, Penalizing Violations thereof and for other purposes
Philippine Health Care Laws
REPUBLIC ACT an act passed by the Congress of the Philippines, while the form of government is Republican
government.
Republic Act 349 Legalizes the use of human organs for surgical, medical and scientific purposes.
Republic Act 1054 Requires the owner, lessee or operator of any commercial, industrial or agricultural
establishment to furnish free emergency, medical and dental assistance to his employees and laborers.
Republic Act 1080 Civil Service Eligibility
Republic Act 1082 Rural Health Unit Act
Republic Act 1136 Act recognizing the Division of Tuberculosis in the DOH
Republic Act 1612 Privilege Tax/Professional tax/omnibus tax should be paid January 31 of each year
Republic Act 1891 Act strengthening Health and Dental services in the rural areas
Republic Act 2382 Philippine Medical Act which regulates the practice of medicines in the Philippines
Republic Act 2644 Philippine Midwifery Act
Republic Act 3573 Law on reporting of Communicable Diseases
Republic Act 4073 Liberalized treatment of Leprosy
Republic Act 4226 Hospital Licensure Act requires all hospital to be licensed before it can operative
Republic Act 5181 Act prescribing permanent residence and reciprocity as qualifications for any examination
or registration for the practice of any profession in the Philippines
Republic Act 5821 The Pharmacy Act
Republic Act 5901 40 hours work for hospital workers
Republic Act 6111 Medicare Act
Republic Act 6365 Established a National Policy on Population and created the Commission on population
Republic Act 6425 Dangerous Drug Act of 1992
Republic Act 6511 Act to standardize the examination and registration fees charged by the National Boards,
and for other purposes.
Republic Act 6675 Generics Act of 1988
Republic Act 6713 Code of Conduct and Ethical Standards for Public Officials and Employees
Republic Act 6725 Act strengthening the prohibition on discrimination against women with respect to
terms and condition of employment
Republic Act 6727 Wage Rationalization Act
Republic Act 6758 Standardized the salaries
Republic Act 6809 Majority age is 18 years old
Republic Act 6972 Day care center in every Barangay
Republic Act 7160 Local Government Code
Republic Act 7164 Philippine Nursing Act of 1991
Republic Act 7170 Law that govern organ donation
Republic Act 7192 Women in development nation building
Republic Act 7277 Magna Carta of Disabled Persons
Republic Act 7305 The Magna Carta of public Health Workers
Republic Act 7392 Philippine Midwifery Act of 1992
Republic Act 7432 Senior Citizen Act
Republic Act 7600 Rooming In and Breastfeeding Act of 1992
Republic Act 7610 Special protection of children against abuse, exploitation and discrimination act
Republic Act 7624 Drug Education Law
Republic Act 7641 New Retirement Law
Republic Act 7658 An act prohibiting the employment of children below 15 years of age
Republic Act 7719 National Blood Service Act of 1994
Republic Act 7875 National Health Insurance Act of 1995
Republic Act 7876 Senior Citizen Center of every Barangay
Republic Act 7877 Anti-sexual harassment Act of 1995
Republic Act 7883 Barangay Health workers Benefits and Incentives Act of 1992
Republic Act 8042 Migrant Workers and Overseas Filipino Act of 1995
Republic Act 8172 Asin Law
Republic Act 8187 Paternity Leave Act of 1995
Republic Act 8203 Special Law on Counterfeit Drugs
Republic Act 8282 Social Security Law of 1997 (amended RA 1161)
Republic Act 8291 Government Service Insurance System Act of 1997 (amended PD 1146)
Republic Act 8344 Hospital Doctors to treat emergency cases referred for treatment
Republic Act 8423 Philippine Institute of Traditional and Alternative Medicine
Republic Act 8424 Personal tax Exemption
Republic Act 8749 The Philippine Clean Air Act of 1999
Republic Act 8981 PRC Modernization Act of 2000
Republic Act 9165 Comprehensive Dangerous Drugs Act 2002
Republic Act 9173 Philippine Nursing Act of 2002
Republic Act 9288 Newborn Screening Act
PRESIDENTIAL DECREE An order of the President. This power of the President which allows him/her to act as
legislators was exercised during the Marshall Law period.
Presidential Decree 46 An act making it punishable for any public officials or employee, whether of the national
or local government, to receive directly or indirectly any gifts or valuable things
Presidential Decree 48 Limits benefits of paid maternity leave privileges to four children
Presidential Decree 69 Limits the number of children to four (4) tax exemption purposes
Presidential Decree 79 Population Commission
Presidential Decree 147 Declares April and May as National Immunization Day
Presidential Decree 148 Regulation on Woman and Child Labor Law
Presidential Decree 166 Strengthened Family Planning program by promoting participation of private sector in
the formulation and implementation of program planning policies.
Presidential Decree 169 Requiring Attending Physician and/or persons treating injuries resulting from any form
of violence.
Presidential Decree 223 Professional Regulation Commission
Presidential Decree 442 Labor Code Promotes and protects employees self-organization and collective
bargaining rights. Provision for a 10% right differential pay for hospital workers.
Presidential Decree 491 Nutrition Program
Presidential Decree 539 Declaring last week of October every as Nurses Week. October 17, 1958
Presidential Decree 541 Allowing former Filipino professionals to practice their respective professions in the
Philippines so they can provide the latent and expertise urgently needed by the homeland
Presidential Decree 568 Role of Public Health midwives has been expanded after the implementation of the
Restructed Health Care Delivery System (RHCDS)
Presidential Decree 603 Child and Youth Welfare Act / Provision on Child Adoption
Presidential Decree 626 Employee Compensation and State Insurance Fund. Provide benefits to person covered
by SSS and GSIS for immediate injury, illness and disability.
Presidential Decree 651 All births and deaths must be registered 30 days after delivery.
Presidential Decree 825 Providing penalty for improper disposal garbage and other forms of uncleanliness and
for other purposes.
Presidential Decree 851 13
th
Month pay
Presidential Decree 856 Code of Sanitation
Presidential Decree 965 Requiring applicants for Marriage License to receive instruction on family planning
and responsible parenthood.
Presidential Decree 996 Provides for compulsory basic immunization for children and infants below 8 years of age.
Presidential Decree 1083 Muslim Holidays
Presidential Decree 1359 A law allowing applicants for Philippine citizenship to take Board Examination
pending their naturalization.
Presidential Decree 1519 Gives medicare benefits to all government employees regardless of status of appointment.
Presidential Decree 1636 requires compulsory membership in the SSS and self-employed
Presidential Decree 4226 Hospital Licensure Act
PROCLAMATION an official declaration by the Chief Executive / Office of the President of the Philippines on
certain programs / projects / situation
Proclamation No.6 UNs goal of Universal Child Immunization; involved NGOs in the immunization program
Proclamation No. 118 Professional regulation Week is June 16 to 22
Proclamation No. 499 National AIDS Awareness Day
Proclamation No. 539 Nurses Week Every third week of October
Proclamation No. 1275 Declaring the third week of October every year as Midwifery Week
LETTER OF INSTRUCTION An order issued by the President to serve as a guide to his/her previous decree
or order.
LOI 47 Directs all school of medicine, nursing, midwifery and allied medical professions and social work to prepare,
plan and implement integration of family planning in their curriculum to require their graduate to take the licensing
examination.
LOI 949 Act on health and health related activities must be integrated with other activities of the overall
national development program. Primary Health Care (10-19-79)
LOI 1000 Government agencies should be given preference to members of the accredited professional
organization when hiring
EXECUTIVE ORDER an order issued by the executive branch of the government in order to implement
a constructional mandate or a statutory provision.
Executive Order 51 The Milk Code
Executive Order 174 National Drug Policy on Availability, Affordability, Safe, Effective and Good Quality drugs
to all
Executive Order 180 Government Workers Collective Bargaining Rights Guidelines on the right to
Organize of government employee.
Executive Order 203 List of regular holidays and special holidays
Executive Order 209 The Family Code (amended by RA 6809)
Executive Order 226 Command responsibility
Executive Order 503 Provides for the rules and regulations implementing the transfer of personnel, assets,
liabilities and records of national agencies whose functions are to be devoted to the local government units.
Executive Order 857 Compulsory Dollar Remittance Law
Other Important Information
Administrative Order 114 Revised/updated the roles and functions of the Municipal Health Officers,
Public Health Nurses and Rural Midwives
ILO Convention 149 Provides the improvement of life and work conditions of nursing personnel.
Primary Health Care (PHC)
Overview
May 1977 -30th World Health Assembly decided that the main health target of the government and WHO is the
attainment of a level of health that would permit them to lead a socially and economically productive life by
the year 2000.
September 6-12, 1978 - First International Conference on PHC in Alma Ata, Russia (USSR) The Alma Ata Declaration
stated that PHC was the key to attain the health for all goal
October 19, 1979 - Letter of Instruction (LOI) 949, the legal basis of PHC was signed by Pres. Ferdinand E. Marcos,
which adopted PHC as an approach towards the design, development and implementation of programs focusing
on health development at community level.
Rationale for Adopting Primary Health Care
Magnitude of Health Problems
Inadequate and unequal distribution of health resources
Increasing cost of medical care
Isolation of health care activities from other development activities
Definition of Primary Health Care
essential health care made universally accessible to individuals and families in the community by means acceptable
to them, through their full participation and at cost that the community can afford at every stage of development.
a practical approach to making health benefits within the reach of all people.
an approach to health development, which is carried out through a set of activities and whose ultimate aim is the
continuous improvement and maintenance of health status
Goal of Primary Health Care
HEALTH FOR ALL FILIPINOS by the year 2000 AND HEALTH IN THE HANDS OF THE PEOPLE by the year
2020.
An improved state of health and quality of life for all people attained through SELF RELIANCE.
Key Strategy to Achieve the Goal:
Partnership with and Empowerment of the people - permeate as the core strategy in the effective provision of
essential health services that are community based, accessible, acceptable, and sustainable, at a cost,
which the community and the government can afford.
Objectives of Primary Health Care
Improvement in the level of health care of the community
Favorable population growth structure
Reduction in the prevalence of preventable, communicable and other disease.
Reduction in morbidity and mortality rates especially among infants and children.
Extension of essential health services with priority given to the underserved sectors.
Improvement in Basic Sanitation
Development of the capability of the community aimed at self- reliance.
Maximizing the contribution of the other sectors for the social and economic development of the community.
Mission
To strengthen the health care system by increasing opportunities and supporting the conditions wherein people
will manage their own health care.
Two Levels of Primary Health Care Workers
1. Barangay Health Workers - trained community health workers or health auxiliary volunteers or traditional birth
attendants or healers.
2. Intermediate level health workers- include the Public Health Nurse, Rural Sanitary Inspector and midwives.
Principles of Primary Health Care
1. 4 A's = Accessibility, Availability, Affordability & Acceptability, Appropriateness of health services.
The health services should be present where the supposed recipients are. They should make use of the available
resources within the community, wherein the focus would be more on health promotion and prevention of illness.
2. Community Participation
heart and soul of PHC
3.People are the center, object and subject of development.
Thus, the success of any undertaking that aims at serving the people is dependent on peoples participation at all
levels of decision-making; planning, implementing, monitoring and evaluating. Any undertaking must also be based on
the peoples needs and problems (PCF, 1990)
Part of the peoples participation is the partnership between the community and the agencies found in the community;
social mobilization and decentralization.
In general, health work should start from where the people are and building on what they have.
Example:
Scheduling of Barangay Health Workers in the health center
Barriers of Community Involvement
o Lack of motivation
o Attitude
o Resistance to change
o Dependence on the part of community people
o Lack of managerial skills
4. Self-reliance
Through community participation and cohesiveness of peoples organization they can generate support for
health care through social mobilization, networking and mobilization of local resources. Leadership and
management skills should be develop among these people. Existence of sustained health care facilities managed
by the people is some of the major indicators that the community is leading to self reliance.
5. Partnership between the community and the health agencies in the provision of quality of life.
Providing linkages between the government and the nongovernment organization and peoples organization.
6. Recognition of interrelationship between the health and development
Health- Is not merely the absence of disease. Neither is it only a state of physical and mental well-being.
Health being a social phenomenon recognizes the interplay of political, socio-cultural and economic factors as its
determinant. Good Health therefore, is manifested by the progressive improvements in the living conditions and
quality of life enjoyed by the community residents (PCF,
Development- is the quest for an improved quality of life for all. Development is multidimensional. It has political,
social, cultural, institutional and environmental dimensions (Gonzales 1994). Therefore, it is measured by the ability
of people to satisfy their basic needs.
7. Social Mobilization
It enhances people participation or governance, support system provided by the Government, networking and
developing secondary leaders.
8. Decentralization
This ensures empowerment and that empowerment can only be facilitated if the administrative structure provides
local level political structures with more substantive responsibilities for development initiators. This also facilities
proper allocation of budgetary resources.
Elements of Primary Health Care
1. Education for Health
Is one of the potent methodologies for information dissemination. It promotes the partnership of both the family
members and health workers in the promotion of health as well as prevention of illness.
2. Locally Endemic Disease Control
The control of endemic disease focuses on the prevention of its occurrence to reduce morbidity rate.
Example Malaria Control and Schistosomiasis Control
3. Expanded Program on Immunization
This program exists to control the occurrence of preventable illnesses especially of children below 6 years old.
Immunizations on poliomyelitis, measles, tetanus, diphtheria and other preventable disease are given for free by the
government and ongoing program of the DOH
4. Maternal and Child Health and Family Planning
The mother and child are the most delicate members of the community. So the protection of the mother and child
to illness and other risks would ensure good health for the community. The goal of Family Planning includes spacing of
children and responsible parenthood.
5. Environmental Sanitation and Promotion of Safe Water Supply
Environmental Sanitation is defined as the study of all factors in the mans environment, which exercise or may
exercise deleterious effect on his well-being and survival. Water is a basic need for life and one factor in mans
environment. Water is necessary for the maintenance of healthy lifestyle. Safe Water and Sanitation is necessary
for basic promotion of health.
6. Nutrition and Promotion of Adequate Food Supply
One basic need of the family is food. And if food is properly prepared then one may be assured healthy family.
There are many food resources found in the communities but because of faulty preparation and lack of knowledge
regarding proper food planning, Malnutrition is one of the problems that we have in the country.
7. Treatment of Communicable Diseases and Common Illness
The diseases spread through direct contact pose a great risk to those who can be infected. Tuberculosis is one of
the communicable diseases continuously occupies the top ten causes of death. Most communicable diseases are also
preventable. The Government focuses on the prevention, control and treatment of these illnesses.
8. Supply of Essential Drugs
This focuses on the information campaign on the utilization and acquisition of drugs.
In response to this campaign, the GENERIC ACT of the Philippines is enacted. It includes the following drugs:
Cotrimoxazole, Paracetamol, Amoxycillin, Oresol, Nifedipine, Rifampicin, INH (isoniazid) and
Pyrazinamide,Ethambutol, Streptomycin,Albendazole,Quinine
Major Strategies of Primary Health Care
1. Elevating Health to a Comprehensive and Sustained National Effort.
Attaining Health for all Filipino will require expanding participation in health and health related programs whether
as service provider or beneficiary. Empowerment to parents, families and communities to make decisions of their
health is really the desired outcome.
Advocacy must be directed to National and Local policy making to elicit support and commitment to major health
concerns through legislations, budgetary and logistical considerations.
2. Promoting and Supporting Community Managed Health Care
The health in the hands of the people brings the government closest to the people. It necessitates a process of
capacity building of communities and organization to plan, implement and evaluate health programs at their levels.
3. Increasing Efficiencies in the Health Sector
Using appropriate technology will make services and resources required for their delivery, effective, affordable,
accessible and culturally acceptable. The development of human resources must correspond to the actual needs of
the nation and the policies it upholds such as PHC. The DOH will continue to support and assist both public and private
institutions particularly in faculty development,
enhancement of relevant curricula and development of standard teaching materials.
4. Advancing Essential National Health Research
Essential National Health Research (ENHR) is an integrated strategy for organizing and managing research using
intersectoral, multi-disciplinary and scientific approach to health programming and delivery.
Four Cornerstones/Pillars in Primary Health Care
1. Active Community Participation
2. Intra and Inter-sectoral Linkages
3. Use of Appropriate Technology
4. Support mechanism made available
Under Five Clinic Program
Overview
The first five years of life form the foundations of the childs physical and mental growth and development.
Studies have shown the mortality and morbidity are high among this age group. The Department of Health established
the Under Five Clinic Program to address this problem.
Program Objectives and Goals
Monitor growth and development of the child until 5 years of age.
Identify factors that may hinder the growth and development of the child.
Activities and Strategies
1. Regular height and weight determination/ monitoring until 5 years old. 0-1 year old=monthly 1 year old and above
=quarterly
2. Recording of immunization, vitamins supplementation, deworming and feeding.
3. Provision of IEC materials (ex. Posters, charts, and toys) that promote and enhance childs proper growth and
development.
4. Provision of a safe and learning oriented environment for the child.
5. Monitoring and Evaluation.
You might also like
- TNCC Study GuideDocument6 pagesTNCC Study Guidekristinekat96% (24)
- Psychotropic Drugs: Bryan Mae H. DegorioDocument65 pagesPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Internal Medicine Quiz 4 DiabetesDocument13 pagesInternal Medicine Quiz 4 DiabetesenzocruzinNo ratings yet
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- A Typology of Nursing Problems in Family Nursing ProblemDocument5 pagesA Typology of Nursing Problems in Family Nursing ProblemRho Vince Caño MalagueñoNo ratings yet
- HSBDocument4 pagesHSBCarlos WebsterNo ratings yet
- NURSING PRACTICE IV Care of Clients With Physiologic and Psychosocial Alterations - RNpediaDocument14 pagesNURSING PRACTICE IV Care of Clients With Physiologic and Psychosocial Alterations - RNpediaBrianMarBeltran100% (1)
- A Typology of Nursing Problems in Family Nursing PracticeDocument10 pagesA Typology of Nursing Problems in Family Nursing PracticeAnika Ajihil100% (2)
- Typology of Nursing Problems in Family Nursing PracticeDocument10 pagesTypology of Nursing Problems in Family Nursing PracticeElaiza Mae MedidasNo ratings yet
- Typology of Nursing Problems in Family Nursing PracticeDocument6 pagesTypology of Nursing Problems in Family Nursing PracticeRonica MendozaNo ratings yet
- S C 7 1 - Mixtures Worksheet and KEYDocument4 pagesS C 7 1 - Mixtures Worksheet and KEYBrianMarBeltran33% (3)
- Nursing Practice I - Foundation of Professional Nursing Practice - RNpediaDocument2 pagesNursing Practice I - Foundation of Professional Nursing Practice - RNpediaBrianMarBeltranNo ratings yet
- Typology of Nursing Care ProblemsDocument2 pagesTypology of Nursing Care ProblemsJohnny Yao JrNo ratings yet
- Three Words Eight LettersDocument509 pagesThree Words Eight Lettersericka_abaya100% (6)
- Separation Techniques WorksheetDocument2 pagesSeparation Techniques WorksheetBrianMarBeltran100% (3)
- Nbme 30 2021 ADocument200 pagesNbme 30 2021 AUsama Bilal100% (3)
- Typology of Nursing Problems in Family Health CareDocument7 pagesTypology of Nursing Problems in Family Health CareJunathan L. DelgadoNo ratings yet
- CT PNSDocument22 pagesCT PNSHany85No ratings yet
- Family Nursing Care Plan. 1st and 2nd Level AssessmentDocument7 pagesFamily Nursing Care Plan. 1st and 2nd Level Assessmentkristel_nicole18yaho100% (1)
- Typology of Family Nursing ProblemDocument9 pagesTypology of Family Nursing ProblemJohn Patrick Leal QuinesNo ratings yet
- Case Study On AnaemiaDocument16 pagesCase Study On AnaemiaLavie Gangwar100% (1)
- The Expectant Dad and First Time Father's GuideFrom EverandThe Expectant Dad and First Time Father's GuideRating: 5 out of 5 stars5/5 (3)
- Typology of Nursing Problems in Family Nursing PracticeDocument10 pagesTypology of Nursing Problems in Family Nursing PracticeJustJ ThingsNo ratings yet
- Case Study Part 2 Patient With Uti (Bag-O)Document48 pagesCase Study Part 2 Patient With Uti (Bag-O)Eaht Quirong0% (1)
- I. Presence of Wellness ConditionDocument9 pagesI. Presence of Wellness ConditionGio Padallan PisquizaNo ratings yet
- CHNDocument120 pagesCHNFaris CruzNo ratings yet
- A Typology of Nursing Problems in Family Nursing PracticeDocument8 pagesA Typology of Nursing Problems in Family Nursing PracticeClifford Ogad0% (1)
- A Typology of Nursing Problems in Family Nursing PracticeDocument9 pagesA Typology of Nursing Problems in Family Nursing PracticeCarrie Joy DecalanNo ratings yet
- Rle 217... Typology of Nursing Problems in Family Nursing Practice MaglayaDocument6 pagesRle 217... Typology of Nursing Problems in Family Nursing Practice MaglayaMakspeyn del Valle - MoonNo ratings yet
- Typology of Nursing Problems in Family Nursing PracticeDocument7 pagesTypology of Nursing Problems in Family Nursing PracticeJoshua PelicanoNo ratings yet
- Saint Paul University Philippines: First Level AssessmentDocument7 pagesSaint Paul University Philippines: First Level AssessmentCLARENCE REMUDARONo ratings yet
- The Family Health Nursing Process 01Document9 pagesThe Family Health Nursing Process 01junald martinNo ratings yet
- Ca CHN Copar ReviewDocument23 pagesCa CHN Copar Reviewapril punzalanNo ratings yet
- A Typology of Nursing Problems in Family Nursing Practice: First Level AssessmentDocument23 pagesA Typology of Nursing Problems in Family Nursing Practice: First Level Assessmentapril punzalanNo ratings yet
- A Typology of Nursing Problems in Family Nursing PracticeDocument9 pagesA Typology of Nursing Problems in Family Nursing PracticeNomelita LoNo ratings yet
- First Level AssessmentDocument9 pagesFirst Level AssessmentGelo IcoNo ratings yet
- Family Nursing Care Plan TypologyDocument6 pagesFamily Nursing Care Plan TypologyLouwella RamosNo ratings yet
- Typology of Nursing Problems in Family Nursing Practice-1Document4 pagesTypology of Nursing Problems in Family Nursing Practice-1Amir PermitivoNo ratings yet
- Family Nursing Care PlanDocument11 pagesFamily Nursing Care PlanDALE DELA CRUZNo ratings yet
- FNCP MaglayaDocument8 pagesFNCP MaglayaVaronNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanneilNo ratings yet
- FamNsgDx 1Document16 pagesFamNsgDx 1Garde PiaoNo ratings yet
- Typology Family Nursing Care PlanDocument9 pagesTypology Family Nursing Care PlanteuuuuNo ratings yet
- CHN A Typology of Nursing Problems in Family Nursing PracticeDocument5 pagesCHN A Typology of Nursing Problems in Family Nursing PracticeRika MaeNo ratings yet
- A Typology of Nursing Problems in Family Nursing PracticeDocument6 pagesA Typology of Nursing Problems in Family Nursing PracticeVince LuzNo ratings yet
- FNCP List of 2nd Level AssessmentDocument5 pagesFNCP List of 2nd Level AssessmentReignallienn Inocencio MartinNo ratings yet
- The Family Nursing Process Is The Same Nursing Process As Applied To The FamilyDocument5 pagesThe Family Nursing Process Is The Same Nursing Process As Applied To The FamilyRobert Dela RiarteNo ratings yet
- Typology of Family Nursing ProblemDocument10 pagesTypology of Family Nursing ProblemRuth PadillaNo ratings yet
- Typology of Nursing Problems FNCPDocument9 pagesTypology of Nursing Problems FNCPPrsnigarbha Dasi D PotianNo ratings yet
- Typhology of Nursing ProblemDocument4 pagesTyphology of Nursing ProblemSteffi AubreyNo ratings yet
- Assessment Database in Family Nursing PracticeDocument4 pagesAssessment Database in Family Nursing PracticeTamayo, Shaina AngelaNo ratings yet
- Typology of Nursing ProblemsDocument39 pagesTypology of Nursing ProblemsAndrea R. NacarioNo ratings yet
- Family Nursing Care PlanDocument78 pagesFamily Nursing Care Planmarielle paezNo ratings yet
- 12 Typology Sample Family Nursing Care PlanDocument8 pages12 Typology Sample Family Nursing Care PlanAven HetutuaNo ratings yet
- Home Visit OrientationDocument29 pagesHome Visit OrientationMay Chelle ErazoNo ratings yet
- CHN 1 Assessment Tools 2021Document6 pagesCHN 1 Assessment Tools 2021Yori Nicole Martine CuyosNo ratings yet
- III. Presence of Health Deficits: O. Others. Specify.Document12 pagesIII. Presence of Health Deficits: O. Others. Specify.Jireh Mae CorderoNo ratings yet
- Level of Assessment FNCPDocument10 pagesLevel of Assessment FNCPLore Anne Mhae SantosNo ratings yet
- File 2022-12-19 14-01-43Document9 pagesFile 2022-12-19 14-01-43Rhea Kathleen MejiaNo ratings yet
- Typology PDFDocument6 pagesTypology PDFCharlaine Gripal SudlaNo ratings yet
- Module 4 Study NotesDocument15 pagesModule 4 Study NotesLia choiNo ratings yet
- Typology of Nursing Problem in Nursing Practice: Tools For AssessmentDocument37 pagesTypology of Nursing Problem in Nursing Practice: Tools For AssessmentIsabel Maxine DavidNo ratings yet
- TYPOLOGY of NURSING PROBLEMS IN FAMILY NURSING PRACTICE and SCALE For Ranking Health Conditions and Problems Accdg To PrioritiesDocument6 pagesTYPOLOGY of NURSING PROBLEMS IN FAMILY NURSING PRACTICE and SCALE For Ranking Health Conditions and Problems Accdg To PrioritiesHarlene Joyce ReyNo ratings yet
- CHN 1 Family Nursing ProcessDocument63 pagesCHN 1 Family Nursing ProcessMark FernandezNo ratings yet
- Typology of Family Nursing Health CareDocument9 pagesTypology of Family Nursing Health Careryujin babieNo ratings yet
- Conclusion:: It TheDocument1 pageConclusion:: It TheMary Grace CuevaNo ratings yet
- Family Nursing Care Plan 1st and 2nd Level AssessmentDocument6 pagesFamily Nursing Care Plan 1st and 2nd Level Assessmenterikajane1357No ratings yet
- Missed Data (FNCP)Document15 pagesMissed Data (FNCP)chesyllemaesultanNo ratings yet
- 5.case Study Format FamilyDocument10 pages5.case Study Format FamilyClay AzunaNo ratings yet
- FNCP List of 1st Level AssessmentDocument6 pagesFNCP List of 1st Level AssessmentReignallienn Inocencio MartinNo ratings yet
- Typology of Nursing ProblemDocument4 pagesTypology of Nursing ProblemCLARISSE CLOIE LAMBERTENo ratings yet
- Helpful Hints...: For Helping Your Child Cope with HospitalizationFrom EverandHelpful Hints...: For Helping Your Child Cope with HospitalizationNo ratings yet
- A Caregivers Plan for Caring for Children & Adults with Special Needs: Navigating Special Needs CareFrom EverandA Caregivers Plan for Caring for Children & Adults with Special Needs: Navigating Special Needs CareNo ratings yet
- Nursing Practice II - Community Health Nursing and Care of The Mother and Child - RNpediaDocument13 pagesNursing Practice II - Community Health Nursing and Care of The Mother and Child - RNpediaBrianMarBeltranNo ratings yet
- TFN NotesDocument83 pagesTFN NotesBrianMarBeltranNo ratings yet
- Lesson Three - Puberty and Body PartsDocument6 pagesLesson Three - Puberty and Body PartsBrianMarBeltranNo ratings yet
- TFN NotesDocument83 pagesTFN NotesBrianMarBeltranNo ratings yet
- Psyche NotesDocument64 pagesPsyche NotesBrianMarBeltranNo ratings yet
- Step 1. Identify The Problem: Nursing ResearchDocument2 pagesStep 1. Identify The Problem: Nursing ResearchBrianMarBeltranNo ratings yet
- NP1 NotesDocument59 pagesNP1 NotesBrianMarBeltranNo ratings yet
- KAD Pada DM Tipe 1Document56 pagesKAD Pada DM Tipe 1hilmiana putriNo ratings yet
- Algoritmo de La Gasometría ArterialDocument15 pagesAlgoritmo de La Gasometría ArterialJhonatan Efraín López CarbajalNo ratings yet
- Anas Umar Internal Defence SlidesDocument23 pagesAnas Umar Internal Defence SlidesAnas UmarNo ratings yet
- Planning and Managing A Dental Continuous Quality Improvement ProjectDocument35 pagesPlanning and Managing A Dental Continuous Quality Improvement ProjecttirahamdillahNo ratings yet
- By Josephine G. Ignacio, MD and Jennifer T. Co, MD, FPOGSDocument9 pagesBy Josephine G. Ignacio, MD and Jennifer T. Co, MD, FPOGSAngela SaldajenoNo ratings yet
- Question For EndoDocument30 pagesQuestion For EndoArti SharmaNo ratings yet
- Clinical Guidelines (Nursing) - Oxygen DeliveryDocument16 pagesClinical Guidelines (Nursing) - Oxygen DeliveryPhan0% (1)
- IMCIDocument17 pagesIMCIapi-3707883No ratings yet
- Calcium Channel BlockersDocument28 pagesCalcium Channel Blockershap hazardNo ratings yet
- 3.1 Midwifery & Gynaecology Nursing Papers QPDocument14 pages3.1 Midwifery & Gynaecology Nursing Papers QPTapobrata Sarkar100% (1)
- Critical Care Nephrology Core Curriculum 2020 PDFDocument18 pagesCritical Care Nephrology Core Curriculum 2020 PDFMartín FleiNo ratings yet
- Post Mature Newborn: Gervacio, Jonah Micah NDocument20 pagesPost Mature Newborn: Gervacio, Jonah Micah NJessa BorreNo ratings yet
- Presentation 5 Hand HygieneDocument26 pagesPresentation 5 Hand HygieneAfeefa Amin AliNo ratings yet
- Assessment 4 (BE)Document9 pagesAssessment 4 (BE)Aryan Judith DoloresNo ratings yet
- Case Study Group C MCN Rle Level IIDocument14 pagesCase Study Group C MCN Rle Level IIRea Jane Astrologo PastorNo ratings yet
- Circulatory System - Babli YadavDocument13 pagesCirculatory System - Babli YadavBabli YadavNo ratings yet
- Ejpd 2018 2 4Document8 pagesEjpd 2018 2 4TikaZyka16No ratings yet
- Diagnosa Icd - 10Document2 pagesDiagnosa Icd - 10Yoery SadewoNo ratings yet
- The Top 15 Best Selling Cancer Drugs in 2022Document16 pagesThe Top 15 Best Selling Cancer Drugs in 2022Soma YasaswiNo ratings yet
- Cashless Authorisation Requisition FormDocument1 pageCashless Authorisation Requisition FormPandurangaNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet