You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- NBME 18 Answers DownloadDocument205 pagesNBME 18 Answers Downloadnashra bukhari76% (33)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- CURRENT Diagnosis & Treatment Gastroenterology, Hepatology, & EndosDocument605 pagesCURRENT Diagnosis & Treatment Gastroenterology, Hepatology, & Endossun seal100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
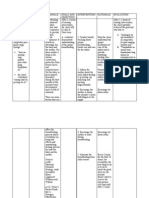
- Ineffective Breast FeedingDocument5 pagesIneffective Breast Feedingcamilleandaj070575% (12)
- Nephrocalcinosis GuideDocument19 pagesNephrocalcinosis GuideRICO NOVYANTONo ratings yet
- Melioidosis in Southern India Epidemiological and Clinical ProfileDocument9 pagesMelioidosis in Southern India Epidemiological and Clinical ProfileMaheshDocherlaNo ratings yet
- Worms in The LiverDocument2 pagesWorms in The LiverMaheshDocherlaNo ratings yet
- Thrombocytopenia in MalariaDocument6 pagesThrombocytopenia in MalariaMaheshDocherlaNo ratings yet
- Spectrum of Hepatic Dysfunction in Enteric FeverDocument2 pagesSpectrum of Hepatic Dysfunction in Enteric FeverMaheshDocherlaNo ratings yet
- Normal Fetal Growth and DevelopmentDocument38 pagesNormal Fetal Growth and DevelopmentArhum SiddiqiNo ratings yet
- Hashimoto's Thyroiditis and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasDocument12 pagesHashimoto's Thyroiditis and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasBashir Mahmud Ellias83% (6)
- Althea NCM 116aDocument192 pagesAlthea NCM 116aspain michaelisNo ratings yet
- Transplantation Tolerance Through Mixed Chimerism. From Allo To XenoDocument11 pagesTransplantation Tolerance Through Mixed Chimerism. From Allo To XenoJose Adriel Chinchay FrancoNo ratings yet
- Sectiuni Si Radiografii - An I, Sem 2Document16 pagesSectiuni Si Radiografii - An I, Sem 2Mihaela456No ratings yet
- Sci 5 PPT q2 WK 1 Day 1-5 (Autosaved)Document93 pagesSci 5 PPT q2 WK 1 Day 1-5 (Autosaved)renato.minaNo ratings yet
- Soalan SainsDocument6 pagesSoalan SainsMohamad HattaNo ratings yet
- Approach To Abnormal Liver Enzymes Whitepaper TI 07106Document6 pagesApproach To Abnormal Liver Enzymes Whitepaper TI 07106luceroNo ratings yet
- Basal GangliaDocument29 pagesBasal Gangliaapi-19916399No ratings yet
- Cardiovascular Notes - All in One FileDocument299 pagesCardiovascular Notes - All in One FileHasan DiabNo ratings yet
- Chamber One-The Neuro Chemistry of Sex-Level 2Document9 pagesChamber One-The Neuro Chemistry of Sex-Level 2Atyeb Ba Atum Re100% (1)
- Endocrine and Urinary SystemDocument5 pagesEndocrine and Urinary SystemShereen ManabilangNo ratings yet
- RRT in ElderlyDocument8 pagesRRT in ElderlySupandy HasanNo ratings yet
- Physiological Functions and Metabolism of Essential Dietary Element IodineDocument4 pagesPhysiological Functions and Metabolism of Essential Dietary Element IodinefitrizeliaNo ratings yet
- Water Balance in Human (Report)Document4 pagesWater Balance in Human (Report)Syairah87No ratings yet
- Solid Organ TransplantationDocument40 pagesSolid Organ TransplantationAkshan SentinelNo ratings yet
- Fisiologi Pengaturan Tekanan Darah SILBERNAGL 2Document6 pagesFisiologi Pengaturan Tekanan Darah SILBERNAGL 221701101016 - Juliana Ayu NugrahaNo ratings yet
- Physioloical Integrity Acute Biologic CrisisDocument42 pagesPhysioloical Integrity Acute Biologic CrisisJohn Paul M. TagapanNo ratings yet
- Heart FailureDocument118 pagesHeart FailureAli Murtaza AbbasNo ratings yet
- Brain Imaging Interpretation GuideDocument67 pagesBrain Imaging Interpretation GuideStefan StefNo ratings yet
- G6-Lesson PlanDocument4 pagesG6-Lesson PlanHansel RamosNo ratings yet
- Introduction of SplanchnologyDocument10 pagesIntroduction of Splanchnologyapi-19916399No ratings yet
- Eye Movement Control and the Role of the Superior ColliculiDocument10 pagesEye Movement Control and the Role of the Superior ColliculiDavis KallanNo ratings yet
- ACCP Farmakoterapi 2013Document296 pagesACCP Farmakoterapi 2013Decy RahmawatiNo ratings yet
- MHC MoleculeDocument45 pagesMHC MoleculeShah NAWAZNo ratings yet
- Iatrogenic Symmastia - Causes and Suggested Repair TechniqueDocument10 pagesIatrogenic Symmastia - Causes and Suggested Repair TechniqueJuan Daniel NaranjoNo ratings yet