You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NIOSH Hazardous DrugsDocument22 pagesNIOSH Hazardous DrugsjimstasonNo ratings yet
- Drugs For Epilepsy: Subgroup 6Document31 pagesDrugs For Epilepsy: Subgroup 6Kwadwo Sarpong JnrNo ratings yet
- Mental Status Exam findingsDocument1 pageMental Status Exam findingsjkfloresNo ratings yet
- Singapore's Merchant Shipping Regulations on Medical StoresDocument36 pagesSingapore's Merchant Shipping Regulations on Medical StoresLoka Radhakrishna NarasaiahNo ratings yet
- Correction of Anterior Crossbite with Removable AppliancesDocument3 pagesCorrection of Anterior Crossbite with Removable Applianceschic organizer100% (1)
- MBChB Year 4 & 5 Past Papers + Answers for Respiratory, Gastrointestinal, Neurology and MoreDocument172 pagesMBChB Year 4 & 5 Past Papers + Answers for Respiratory, Gastrointestinal, Neurology and MoreHariharan NarendranNo ratings yet
- Amen ADD QuestionnaireDocument3 pagesAmen ADD QuestionnaireReeshabhdev GauttamNo ratings yet
- Fpsyt 13 1049476Document12 pagesFpsyt 13 1049476putriNo ratings yet
- Dharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDocument8 pagesDharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDr. Krishna N. SharmaNo ratings yet
- Bacillary Dysentery (ShigellosisDocument2 pagesBacillary Dysentery (ShigellosisZam PamateNo ratings yet
- Ebola Virus Disease: Causes, Symptoms and TreatmentDocument15 pagesEbola Virus Disease: Causes, Symptoms and TreatmentAlvin AlmazanNo ratings yet
- Tress Test: The Gale Encyclopedia of MedicineDocument7 pagesTress Test: The Gale Encyclopedia of MedicineSalsabilla KimikoNo ratings yet
- Psychosis NosDocument8 pagesPsychosis Nosapi-253211220No ratings yet
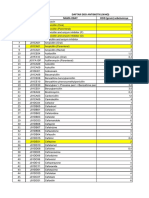
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDocument12 pagesDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaNo ratings yet
- OSCE Counselling NotesDocument3 pagesOSCE Counselling NotesjuweriyNo ratings yet
- IHI Global Trigger ToolDocument46 pagesIHI Global Trigger ToolJuan Manuel LujanNo ratings yet
- Intramuscular CKLDocument2 pagesIntramuscular CKLapi-310181843No ratings yet
- Nursing Process Mcqs Session by Husain.ZDocument14 pagesNursing Process Mcqs Session by Husain.ZInam ullah KhanNo ratings yet
- Disease Prevention Primary Secondary TertiaryDocument1 pageDisease Prevention Primary Secondary TertiaryprogramgrabberNo ratings yet
- Complicatii Si Sechele Tardive Dupa Tratamentul Multimodal Al GlioamelorDocument35 pagesComplicatii Si Sechele Tardive Dupa Tratamentul Multimodal Al GlioamelorBiblioteca CSNTNo ratings yet
- Solvalitt Aluminium - MSDSDocument11 pagesSolvalitt Aluminium - MSDSLITOGENT 893No ratings yet
- Myocardial Infarction Causes, Symptoms, TreatmentDocument23 pagesMyocardial Infarction Causes, Symptoms, TreatmentAnelle Umali50% (2)
- Satanic Ritual Abuse Evidence and ArticlesDocument16 pagesSatanic Ritual Abuse Evidence and Articlessmartnews100% (3)
- Ielts Reading Test 17Document8 pagesIelts Reading Test 17Trương Thuận KiệtNo ratings yet
- Bed Number TenDocument7 pagesBed Number Tenapi-444163791No ratings yet
- Platelet-Rich Plasma For Hair Restoration: Natalie Justicz,, Adeeb Derakhshan,, Jenny X. Chen,, Linda N. LeeDocument7 pagesPlatelet-Rich Plasma For Hair Restoration: Natalie Justicz,, Adeeb Derakhshan,, Jenny X. Chen,, Linda N. Leejaviers45No ratings yet
- Septic ArthritisDocument8 pagesSeptic ArthritisLorebell100% (2)
- Polydactyly of The Foot A Review.92Document10 pagesPolydactyly of The Foot A Review.92mamyeu1801No ratings yet
- FMST 314 Finals NotesDocument8 pagesFMST 314 Finals NotesmoomoomaoNo ratings yet
- Ot ProtocolDocument38 pagesOt ProtocolSelva KumarNo ratings yet