You might also like
- 10+0 Point Agenda of President Rodrigo DuterteDocument20 pages10+0 Point Agenda of President Rodrigo DuterteYkskciv Ced Prince100% (1)
- Salient Features: Philippine Climate Change ACT - RA 9729Document29 pagesSalient Features: Philippine Climate Change ACT - RA 9729JO HN Scuba-rNo ratings yet
- LGU Tupi - Citizens CharterDocument72 pagesLGU Tupi - Citizens CharterLouie ManansalaNo ratings yet
- Different Faces of Filipino Administrative Culture PDFDocument13 pagesDifferent Faces of Filipino Administrative Culture PDFTessa Tacata100% (1)
- Public Fiscal Administration TestDocument7 pagesPublic Fiscal Administration TestApril Dominguez-Benzon100% (2)
- Salient Features of RA 10587 FinalDocument32 pagesSalient Features of RA 10587 Finalboen jayme100% (1)
- Town and Gown ApproachDocument31 pagesTown and Gown Approachgerald sanchezNo ratings yet
- Ethics Ra 6713 PDFDocument47 pagesEthics Ra 6713 PDFVanessa Obra Do100% (4)
- Local Autonomy in The PhilippinesDocument8 pagesLocal Autonomy in The PhilippinesRonn Briane AtudNo ratings yet
- Advantages and Disadvantages of Local Autonomy 20160905Document7 pagesAdvantages and Disadvantages of Local Autonomy 20160905grassNo ratings yet
- What Is The Difference Between Graft and CorruptionDocument3 pagesWhat Is The Difference Between Graft and CorruptionPrince Khalid67% (3)
- Good Governance in The Philippines ArticleDocument3 pagesGood Governance in The Philippines ArticleLiz80% (5)
- Action Research On The Implementation of The Anti-Red Tape Act of 2007Document33 pagesAction Research On The Implementation of The Anti-Red Tape Act of 2007JN Dela Peña50% (8)
- Philippine Administrative SystemDocument7 pagesPhilippine Administrative SystemEd Villa50% (2)
- Local Government AdministrationDocument35 pagesLocal Government AdministrationTeriote Edeliza100% (1)
- Mejillano - Critique Paper (RA 9729)Document10 pagesMejillano - Critique Paper (RA 9729)Criselle MejillanoNo ratings yet
- Republic Act No. 3019 Anti-Graft and Corrupt Practices ActDocument32 pagesRepublic Act No. 3019 Anti-Graft and Corrupt Practices ActJaner Sanchez100% (2)
- The Development of Public Finance InstitutionsDocument49 pagesThe Development of Public Finance InstitutionsPeo Batangasph100% (3)
- Hacienda Luisita Problems and SolutionsDocument7 pagesHacienda Luisita Problems and Solutionsangelo prietoNo ratings yet
- Katarungang PambarangayDocument32 pagesKatarungang PambarangayRLO1100% (1)
- Tools For Implementing The Comprehensive Land Use PlanDocument11 pagesTools For Implementing The Comprehensive Land Use Planmarwinjs100% (3)
- Philippine Administrative SystemDocument5 pagesPhilippine Administrative SystemSalveMay DumlaoNo ratings yet
- 2019 Public Policy and Program AdministrationDocument9 pages2019 Public Policy and Program AdministrationCzar Jose Benavente100% (1)
- DENR History Vision and MissionDocument6 pagesDENR History Vision and Missionjofel delicanaNo ratings yet
- Salient Features of The Local Government CodeDocument10 pagesSalient Features of The Local Government CodeJasmin Beloya100% (1)
- Lecture 10 - Local Government Administration 1Document15 pagesLecture 10 - Local Government Administration 1Dioscoroo NunezNo ratings yet
- Salient Features of Ra 6713Document2 pagesSalient Features of Ra 6713Kathleen Kaye Concha100% (1)
- 03 DOH Red Orchid Awards (Batch 1)Document46 pages03 DOH Red Orchid Awards (Batch 1)VikangAdor100% (1)
- Theories and PracticeDocument41 pagesTheories and PracticeJessie Jean Condez Mangilaya100% (5)
- Agrarian Law Lesson 1Document6 pagesAgrarian Law Lesson 1rapturereadyNo ratings yet
- A Research Paper Anti Red Tape ActDocument18 pagesA Research Paper Anti Red Tape ActMara Cojamco50% (2)
- Answer - Local Government CG - lq3Document8 pagesAnswer - Local Government CG - lq3Reymond IgayaNo ratings yet
- Taxation in The PhilippinesDocument36 pagesTaxation in The PhilippinesGail Delima100% (1)
- History and Evolution of Philippine Local Government and AdministrationDocument10 pagesHistory and Evolution of Philippine Local Government and AdministrationGiann Lorrenze Famisan Ragat100% (1)
- Local Fiscal AdministrationDocument18 pagesLocal Fiscal AdministrationLander Dean S. ALCORANONo ratings yet
- Davao Oriental: Local Policies On Disaster Risk Reduction, Climate Change Adaptation and Food and Nutrition SecurityDocument37 pagesDavao Oriental: Local Policies On Disaster Risk Reduction, Climate Change Adaptation and Food and Nutrition Securitycarlos-tulali-1309100% (2)
- Local Government Code of 1991 (Updated)Document218 pagesLocal Government Code of 1991 (Updated)Arahbells100% (2)
- BFP Caloocan HistoryDocument8 pagesBFP Caloocan Historytorrazo100% (1)
- Bida ProgramDocument19 pagesBida ProgramJose, Alyssa JeanNo ratings yet
- Ethics and Accountability The Philippine Experrience by CSCDocument5 pagesEthics and Accountability The Philippine Experrience by CSCLinda Himoldang Marcaida100% (2)
- RA NR 9745Document22 pagesRA NR 9745Diadem Glace BaldadoNo ratings yet
- Local Fiscal AdministrationDocument12 pagesLocal Fiscal AdministrationJanice Aguila Suarez - Madarang100% (1)
- Issues & Problems in Public AdministrationDocument12 pagesIssues & Problems in Public AdministrationRosalvie Dante86% (7)
- Philippine Administrative Thought and Institutions - Garcia - TolentinoDocument107 pagesPhilippine Administrative Thought and Institutions - Garcia - TolentinoRochene Garcia86% (58)
- Salient Features of 9700Document16 pagesSalient Features of 9700histosol100% (1)
- Authority Levers For Implementing The CLUPDocument10 pagesAuthority Levers For Implementing The CLUPErnie Gultiano100% (1)
- Salient Features of CARLDocument4 pagesSalient Features of CARLColeen Navarro-RasmussenNo ratings yet
- Ethics and Accountability: The Philippine ExperienceDocument55 pagesEthics and Accountability: The Philippine ExperienceLerwin GaringaNo ratings yet
- Philippine Administrative Thoughts and Institution Module 1Document1 pagePhilippine Administrative Thoughts and Institution Module 1Jermaine Manalo Parilla75% (4)
- Pa 103 Philippine Administrative Thoughts and Institutions Module 5 EndtermDocument12 pagesPa 103 Philippine Administrative Thoughts and Institutions Module 5 EndtermLö Räine AñascoNo ratings yet
- Local Fiscal Administration: Gilbert R. HufanaDocument27 pagesLocal Fiscal Administration: Gilbert R. Hufanagilberthufana446877100% (1)
- MODULE 1 Overview of Public Fiscal AdministrationDocument8 pagesMODULE 1 Overview of Public Fiscal AdministrationRica GalvezNo ratings yet
- Tertiary Education Subsidy Sharing AgreementDocument2 pagesTertiary Education Subsidy Sharing AgreementPark Shin HyeNo ratings yet
- Ra9485 Anti-Red Tape Act of 2007Document6 pagesRa9485 Anti-Red Tape Act of 2007sydmarielle100% (1)
- Reforming The Bureaucracy Can Citizen ParticipateDocument4 pagesReforming The Bureaucracy Can Citizen ParticipateAbegail Dumadag100% (1)
- Factors Influencing The Quality of Healt PDFDocument5 pagesFactors Influencing The Quality of Healt PDFIsaacNo ratings yet
- Debate LinesDocument4 pagesDebate LinesLyte LightNo ratings yet
- Ao2021 0006Document9 pagesAo2021 0006Elredd ArtNo ratings yet
- Health RefomsDocument11 pagesHealth RefomsDr. Muhammad Zaman ZahidNo ratings yet
- Khyber Pakhtunkhwa Health Sector Review: Hospital CareFrom EverandKhyber Pakhtunkhwa Health Sector Review: Hospital CareNo ratings yet
- Urban Governance: Topic GuideDocument60 pagesUrban Governance: Topic GuideSaifuddin SidikiNo ratings yet
- Unit 9 Lesson 1 Decentralization and Local GovernanceDocument16 pagesUnit 9 Lesson 1 Decentralization and Local GovernancePatrixia Miclat100% (1)
- Presentation Human Rights ConceptsDocument11 pagesPresentation Human Rights ConceptsmaliksuneelNo ratings yet
- DecentralizationDocument20 pagesDecentralizationLaurens BuloNo ratings yet
- Federalism: Q1. What Is Federalism?Document4 pagesFederalism: Q1. What Is Federalism?AadarshNo ratings yet
- "The Gandhian Approach To Rural Development: IJCRT1133061 59Document12 pages"The Gandhian Approach To Rural Development: IJCRT1133061 59Anirban KunduNo ratings yet
- SSRN Id2580664Document58 pagesSSRN Id2580664ashishgupta09100% (1)
- A Bottom Up Approach To Cultural Policy MakingDocument66 pagesA Bottom Up Approach To Cultural Policy MakingKatarina PavićNo ratings yet
- Good Governance in Ethiopia PDFDocument3 pagesGood Governance in Ethiopia PDFKate100% (3)
- Atty. Aloi Renz P. Santos: Attorney IV, Commission On Human Rights III 09154952774/ 09255682611 TW/IG: @aloi - SantosDocument35 pagesAtty. Aloi Renz P. Santos: Attorney IV, Commission On Human Rights III 09154952774/ 09255682611 TW/IG: @aloi - SantosAngelica TalledoNo ratings yet
- Empire Case 2 OutstandingDocument23 pagesEmpire Case 2 OutstandingHash100% (1)
- Messari Report Eth2 The Next Evolution of CryptoeconomyDocument70 pagesMessari Report Eth2 The Next Evolution of Cryptoeconomyfabio menghiNo ratings yet
- Notes FederalismDocument11 pagesNotes FederalismSmita ChandraNo ratings yet
- Discover, Use and Analyze Decentralized Apps in The World's Largest Dapp StoreDocument25 pagesDiscover, Use and Analyze Decentralized Apps in The World's Largest Dapp StoreBrendon SoongNo ratings yet
- 0307 Research SpotlightDocument7 pages0307 Research SpotlightSaina ChuhNo ratings yet
- Asha DissertationDocument73 pagesAsha DissertationBrooke TillmanNo ratings yet
- Buisiness StudiesDocument7 pagesBuisiness Studiessainiaarti0181No ratings yet
- Managing The Forces of FragmentationDocument9 pagesManaging The Forces of FragmentationJosua PranataNo ratings yet
- Conflict Resolution - Theories and PracticeDocument25 pagesConflict Resolution - Theories and Practicejaseme7579No ratings yet
- Contingency Theory PDFDocument12 pagesContingency Theory PDFRichard WangNo ratings yet
- National Agricultural Sector Extension 2012Document55 pagesNational Agricultural Sector Extension 2012dan yaganNo ratings yet
- Decentralization StrategyDocument25 pagesDecentralization StrategyNino BakhiaNo ratings yet
- UNIT 3.2 Centralization and DecentralizationDocument7 pagesUNIT 3.2 Centralization and DecentralizationHOD ECENo ratings yet
- Decentralisation A Decade of Kerala ExperienceDocument41 pagesDecentralisation A Decade of Kerala ExperienceJoshy JosephNo ratings yet
- Comparative Decentralization Lessons From Pakistan Indonesia and The PhilippinesDocument15 pagesComparative Decentralization Lessons From Pakistan Indonesia and The PhilippinesSaif Ullah Zehri50% (2)
- Unpacking Local Economic Development: A Case Study From Nekemte Town and Its Hinterlands, Oromia, EthiopiaDocument15 pagesUnpacking Local Economic Development: A Case Study From Nekemte Town and Its Hinterlands, Oromia, Ethiopiafetene birruNo ratings yet
- Application With Example - Henri FayolDocument3 pagesApplication With Example - Henri FayolVAI ProcurementNo ratings yet
- Understanding Vulnerability III Module 7Document19 pagesUnderstanding Vulnerability III Module 7HKANo ratings yet
- Centralized ProcurementDocument18 pagesCentralized Procurementkarthik rNo ratings yet
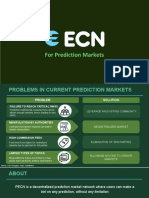
- For Prediction MarketsDocument21 pagesFor Prediction Marketsmaheshwar billaNo ratings yet