You might also like
- Metanalise Lowback PainDocument11 pagesMetanalise Lowback PainGabriel Gaspar Bike FitNo ratings yet
- Cochranne Low Back Pain NsaidDocument151 pagesCochranne Low Back Pain NsaidGabriel Gaspar Bike FitNo ratings yet
- Radiosteriometric Analysis of Movement in The Sacroiliac Joint During A Single-Leg Stance in Patients With Long-Lasting Pelvic Girdle PainDocument7 pagesRadiosteriometric Analysis of Movement in The Sacroiliac Joint During A Single-Leg Stance in Patients With Long-Lasting Pelvic Girdle PainGabriel Gaspar Bike FitNo ratings yet
- 8912 PDFDocument104 pages8912 PDFGabriel Gaspar Bike FitNo ratings yet
- Diagnosis of Sacroiliac Joint Pain: Validity of Individual Provocation Tests and Composites of TestsDocument12 pagesDiagnosis of Sacroiliac Joint Pain: Validity of Individual Provocation Tests and Composites of TestsGabriel Gaspar Bike FitNo ratings yet
- Validity of McKenzie exam and SI joint testsDocument9 pagesValidity of McKenzie exam and SI joint testsGabriel Gaspar Bike FitNo ratings yet
- Sacroiliac Joint Pain Referral ZonesDocument5 pagesSacroiliac Joint Pain Referral ZonesGabriel Gaspar Bike FitNo ratings yet
- A Radiostereometric Analysis of Movements of The Sacroiliac Joints During The Standing Hip Flexion TestDocument5 pagesA Radiostereometric Analysis of Movements of The Sacroiliac Joints During The Standing Hip Flexion TestGabriel Gaspar Bike FitNo ratings yet
- Sacroiliac Joint Pain: A Comprehensive Review of Anatomy, Diagnosis, and TreatmentDocument14 pagesSacroiliac Joint Pain: A Comprehensive Review of Anatomy, Diagnosis, and TreatmentGabriel Gaspar Bike FitNo ratings yet
- A Radiostereometric Analysis of Movements of The Sacroiliac Joints During The Standing Hip Flexion TestDocument5 pagesA Radiostereometric Analysis of Movements of The Sacroiliac Joints During The Standing Hip Flexion TestGabriel Gaspar Bike FitNo ratings yet
- LINKSDocument1 pageLINKSGabriel Gaspar Bike FitNo ratings yet
- ENDOMETRIOSE X FISIOTERAPIA PDFDocument19 pagesENDOMETRIOSE X FISIOTERAPIA PDFLuiza GusmãoNo ratings yet
- Concept Version: European Guidelines On The Diagnosis and Treatment of Pelvic Girdle PainDocument50 pagesConcept Version: European Guidelines On The Diagnosis and Treatment of Pelvic Girdle PainGabriel Gaspar Bike FitNo ratings yet
- Journal Of: The Sacroiliac Joint: An Overview of Its Anatomy, Function and Potential Clinical ImplicationsDocument31 pagesJournal Of: The Sacroiliac Joint: An Overview of Its Anatomy, Function and Potential Clinical ImplicationsGabriel Gaspar Bike FitNo ratings yet
- Pelvic Pain During Pregnancy Is Associated With Asymmetric Laxity of The Sacroiliac JointsDocument6 pagesPelvic Pain During Pregnancy Is Associated With Asymmetric Laxity of The Sacroiliac JointsGabriel Gaspar Bike FitNo ratings yet
- Nihms 695755 PDFDocument29 pagesNihms 695755 PDFGabriel Gaspar Bike FitNo ratings yet
- Still ReviewDocument24 pagesStill ReviewGabriel Gaspar Bike Fit100% (1)
- Prevalence of Myofascial Trigger Points in Spinal Disorders: A Systematic Review and Meta-AnalysisDocument22 pagesPrevalence of Myofascial Trigger Points in Spinal Disorders: A Systematic Review and Meta-AnalysisGabriel Gaspar Bike FitNo ratings yet
- Fatigue Effects On The Coordinative Pattern During CyclingDocument6 pagesFatigue Effects On The Coordinative Pattern During CyclingGabriel Gaspar Bike FitNo ratings yet
- Custom Formed Orthoses in CyclingDocument6 pagesCustom Formed Orthoses in CyclingGabriel Gaspar Bike FitNo ratings yet
- Estabilidade Do CORE - CICLISMODocument3 pagesEstabilidade Do CORE - CICLISMOGabriel Gaspar Bike FitNo ratings yet
- Low-Tech Running Shoes in High DemandDocument1 pageLow-Tech Running Shoes in High DemandGabriel Gaspar Bike FitNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Back Spine AnatomyDocument3 pagesBack Spine AnatomyNinjaNo ratings yet
- TO Splenectomy 2Document31 pagesTO Splenectomy 2sphericalfaNo ratings yet
- Qimen Liv-14: Liver Channel 1Document2 pagesQimen Liv-14: Liver Channel 1ray72roNo ratings yet
- Radio - GitDocument19 pagesRadio - GitVon HippoNo ratings yet
- GI Anatomy Practice QuestionsDocument6 pagesGI Anatomy Practice QuestionsFaddy OrahaNo ratings yet
- Abdominal Exam GuideDocument9 pagesAbdominal Exam GuideDarawan MirzaNo ratings yet
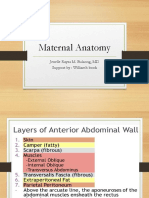
- Maternal Anatomy WilliamsDocument60 pagesMaternal Anatomy WilliamsZari Novela100% (2)
- Biomechanics of The Vertebral ColumnDocument44 pagesBiomechanics of The Vertebral ColumnVijay PradeepNo ratings yet
- GENITAL PROLAPSE GUIDEDocument58 pagesGENITAL PROLAPSE GUIDEsushma nakkinaNo ratings yet
- Chapter 11 The Cardiovascular SystemDocument25 pagesChapter 11 The Cardiovascular SystemYeshia InocencioNo ratings yet
- Diaphragm: Mr. Abdur Rehman BS-cardiology Kmu-IpmsDocument19 pagesDiaphragm: Mr. Abdur Rehman BS-cardiology Kmu-IpmsAbdurrehman SafiNo ratings yet
- Overview of Scoliosis & Clinical AssessmentDocument57 pagesOverview of Scoliosis & Clinical AssessmentmilaNo ratings yet
- Bones of The NeckDocument24 pagesBones of The NeckSmartyna SophiaNo ratings yet
- Logarajah, 2021Document6 pagesLogarajah, 2021Aze Andrea PutraNo ratings yet
- Medical Terminlogy Body Planes SectionsDocument75 pagesMedical Terminlogy Body Planes SectionsSTEM-G.04 Kiarrah Katrina BotinNo ratings yet
- International Journal of Veterinary Science and MedicineDocument6 pagesInternational Journal of Veterinary Science and MedicineXinevlin XinevlinNo ratings yet
- Lung Collapse: A Review: Dr. Girish Kukade Radiology Department, AFHDocument61 pagesLung Collapse: A Review: Dr. Girish Kukade Radiology Department, AFHkukadegirishNo ratings yet
- Mrcs Part B Osce-AnatomyDocument392 pagesMrcs Part B Osce-AnatomyWaeel Hamouda100% (3)
- OIA Muscles of The CatDocument3 pagesOIA Muscles of The CatAyee AtienzaNo ratings yet
- Professional English in Use - MedicineDocument244 pagesProfessional English in Use - MedicineAlbeliz CordobaNo ratings yet
- Anatomy of GI TractDocument24 pagesAnatomy of GI TractMuhammad Ade RahmanNo ratings yet
- 06 - 07 - Anatomy of The Chest Wall and BreastDocument16 pages06 - 07 - Anatomy of The Chest Wall and Breastbo gum parkNo ratings yet
- Student Guide To The Frog DissectionDocument3 pagesStudent Guide To The Frog Dissectionapi-233187566No ratings yet
- The Inner UnitDocument6 pagesThe Inner UnitsololuiNo ratings yet
- Acute Abdomen SeriesssDocument44 pagesAcute Abdomen SeriesssSupitcha ThongchaiNo ratings yet
- Tugas Ekspertise AbdomenDocument42 pagesTugas Ekspertise AbdomentriaclaresiaNo ratings yet
- Chapter 13 - Blood Vessels and CirculationDocument21 pagesChapter 13 - Blood Vessels and CirculationGabriel CastenNo ratings yet
- Female Reproductive Organs OverviewDocument31 pagesFemale Reproductive Organs OverviewSabita PaudelNo ratings yet
- Urogenital PainDocument282 pagesUrogenital PainAlex YoungNo ratings yet
- Lesson 1 Human Breathing SystemDocument37 pagesLesson 1 Human Breathing SystemDavid Lawrence GarciaNo ratings yet