You might also like
- Circadian Rhythm Reset for Better Sleep and MetabolismDocument22 pagesCircadian Rhythm Reset for Better Sleep and Metabolismfyrtenheimer100% (1)
- Weight Training: A Beginners Guide to Building a Leaner, Bigger, Stronger Body, Naturally and EasilyFrom EverandWeight Training: A Beginners Guide to Building a Leaner, Bigger, Stronger Body, Naturally and EasilyRating: 5 out of 5 stars5/5 (5)
- Cancer Is DEAD Cancer Cures From A To ZDocument169 pagesCancer Is DEAD Cancer Cures From A To Zcamjob80% (5)
- Autoimmune Matrix DR Peter Osborne EbookDocument68 pagesAutoimmune Matrix DR Peter Osborne EbookSoftMan100% (1)
- Secrets of Mind Body HealingDocument17 pagesSecrets of Mind Body Healingtemporal130100% (1)
- Natures.n1 Healing - SecretDocument29 pagesNatures.n1 Healing - Secretwikorv8497No ratings yet
- Deep Muscle Therapy 1 Intro 06Document33 pagesDeep Muscle Therapy 1 Intro 06Enyaw DroffatsNo ratings yet
- Biology PDFDocument29 pagesBiology PDFThePhantomStranger100% (1)
- The Heart of Flow PDFDocument72 pagesThe Heart of Flow PDFBenjamin Rüffin100% (2)
- Energy Blueprint 4 Secrets To Fatigue 6 Science Backed Strategies To Dramatically Increase Your EnergyDocument32 pagesEnergy Blueprint 4 Secrets To Fatigue 6 Science Backed Strategies To Dramatically Increase Your EnergyFuerza VitalNo ratings yet
- Vagus Nerve Exercises To Rewire Your Brain: Stimulate Your Vagus Nerve With Natural Self-Healing Daily Exercises For Anxiety, Depression, Trauma & OverthinkingFrom EverandVagus Nerve Exercises To Rewire Your Brain: Stimulate Your Vagus Nerve With Natural Self-Healing Daily Exercises For Anxiety, Depression, Trauma & OverthinkingNo ratings yet
- 3 Interview Transcripts From The Superhuman Energy SummitDocument54 pages3 Interview Transcripts From The Superhuman Energy SummitFuerza VitalNo ratings yet
- Joe Rozencwajg InterviewDocument17 pagesJoe Rozencwajg InterviewGold SunriseNo ratings yet
- The Uplink: Issue No.5Document2 pagesThe Uplink: Issue No.5taichi7No ratings yet
- Patho Supplement Handout For Sept 2018 UPDATED May 2018 PDFDocument25 pagesPatho Supplement Handout For Sept 2018 UPDATED May 2018 PDFemely p. tango100% (1)
- Chronic Fatigue: Defeating Permanent Fatigue and Starting the Day with Renewed StrengthFrom EverandChronic Fatigue: Defeating Permanent Fatigue and Starting the Day with Renewed StrengthRating: 5 out of 5 stars5/5 (2)
- Klinghardt Introduction To Light and The Human BiofieldDocument14 pagesKlinghardt Introduction To Light and The Human BiofieldPoorni ShivaramNo ratings yet
- Healthy, Happy Gut Summit™: Everything You Need To Know About Probiotics Michael RuscioDocument15 pagesHealthy, Happy Gut Summit™: Everything You Need To Know About Probiotics Michael RuscioMiha VucNo ratings yet
- Auto Immune Disease and Fibromyalgia: The Traumatic Brain Injury Connection: TRAUMATIC BRAIN INJURY: TBI & POST-CONCUSSION SYNDOME: PCS, #3From EverandAuto Immune Disease and Fibromyalgia: The Traumatic Brain Injury Connection: TRAUMATIC BRAIN INJURY: TBI & POST-CONCUSSION SYNDOME: PCS, #3No ratings yet
- CH Dreaming NeurogenesisDocument31 pagesCH Dreaming NeurogenesisrommelsousaNo ratings yet
- Homeo TipsDocument146 pagesHomeo TipsBalaji Siddhu100% (2)
- Homeo TipsDocument124 pagesHomeo TipsAditya uniyal100% (2)
- Lesson: Dr. Leon Hammer, M.DDocument14 pagesLesson: Dr. Leon Hammer, M.DRocío JMNo ratings yet
- Secrets of Mind Body HealingDocument19 pagesSecrets of Mind Body HealingCarolBhagavatiMcDonnellNo ratings yet
- The Thyroid SolutionDocument21 pagesThe Thyroid SolutionJosh Bill100% (1)
- Diagnosing and treating chronic stressDocument8 pagesDiagnosing and treating chronic stressAlex Maric Dragas100% (1)
- Chronic Fatigue: Defeating Permanent Fatigue and Starting the Day with Renewed Strength (Chronic Fatigue Syndrome, Tiredness, Burnout)From EverandChronic Fatigue: Defeating Permanent Fatigue and Starting the Day with Renewed Strength (Chronic Fatigue Syndrome, Tiredness, Burnout)No ratings yet
- The Whole Brain Diet: the microbiome solution to heal depression, anxiety, and mental fog without prescription drugsFrom EverandThe Whole Brain Diet: the microbiome solution to heal depression, anxiety, and mental fog without prescription drugsNo ratings yet
- DR Sarno Free - Report - 11!09!11Document9 pagesDR Sarno Free - Report - 11!09!11Crisalcala100% (3)
- Heal Yourself in 15 DaysDocument37 pagesHeal Yourself in 15 DaysAtma Love100% (3)
- Migraines and Epilepsy: How to Find Relief, Live Well, and Protect Your BrainFrom EverandMigraines and Epilepsy: How to Find Relief, Live Well, and Protect Your BrainNo ratings yet
- You Are Your Own Best Medicine: A Doctor's Advice on the Body's Natural Healing PowersFrom EverandYou Are Your Own Best Medicine: A Doctor's Advice on the Body's Natural Healing PowersRating: 4 out of 5 stars4/5 (2)
- Pandemics Have Occurred Throughout The DecadesDocument4 pagesPandemics Have Occurred Throughout The DecadesPhiNo LupHt DindudNo ratings yet
- The Importance of Symptomatic Treatment 1376187581Document4 pagesThe Importance of Symptomatic Treatment 1376187581giullianosilva4874No ratings yet
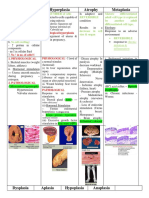
- Understanding Atrophy, Hypertrophy and HyperplasiaDocument30 pagesUnderstanding Atrophy, Hypertrophy and HyperplasiaFiras Anaya100% (1)
- Medical English: Explaining Investigations and ProceduresDocument41 pagesMedical English: Explaining Investigations and Proceduresfiorella lombardiNo ratings yet
- Q: What Are The Origins of The Stress Response?Document5 pagesQ: What Are The Origins of The Stress Response?Ser Jhun ChangNo ratings yet
- Facing Neu Ent Fearlessly: Ro AssessmDocument7 pagesFacing Neu Ent Fearlessly: Ro AssessmokipashaNo ratings yet
- Article On CellsDocument5 pagesArticle On CellsCad NoviceNo ratings yet
- Antiepileptic Drugs Guide: Seizure Causes & MedicationsDocument15 pagesAntiepileptic Drugs Guide: Seizure Causes & MedicationsTod KembleNo ratings yet
- Mast Cell Activation Syndrome - The Functional Medicine ApproachDocument34 pagesMast Cell Activation Syndrome - The Functional Medicine Approach0xcffaaNo ratings yet
- Power Over Suffering: Discovering and Overcoming Hidden Sources of PainFrom EverandPower Over Suffering: Discovering and Overcoming Hidden Sources of PainNo ratings yet
- Introduction To Biology 1Document17 pagesIntroduction To Biology 1Samuel PonceNo ratings yet
- Mindfulness Health Benefits of MeditationDocument6 pagesMindfulness Health Benefits of MeditationDaniel BustamanteNo ratings yet
- Fasting Can Save Your Life and Multiple SclerosisDocument3 pagesFasting Can Save Your Life and Multiple SclerosisJonas Sunshine Callewaert100% (1)
- Emu Sept 2013 Part 2Document28 pagesEmu Sept 2013 Part 2jbrazg84No ratings yet
- Free Somatics: Reawakening The Minds Control of Movement, Flexibility, and Health PDFDocument6 pagesFree Somatics: Reawakening The Minds Control of Movement, Flexibility, and Health PDFRajesh S VNo ratings yet
- Index: 22/8/14 1 Natural Happiness: The Truth About Exercise and DepressionDocument11 pagesIndex: 22/8/14 1 Natural Happiness: The Truth About Exercise and DepressionSiliconNo ratings yet
- Wild Horses - The Stress of CaptivityDocument16 pagesWild Horses - The Stress of CaptivityAmerican Wild Horse PreservationNo ratings yet
- Nikolai Amosov's Anti-Aging GymnasticsDocument3 pagesNikolai Amosov's Anti-Aging Gymnasticsmladen1858948No ratings yet
- NeurologyDocument15 pagesNeurologyed192kbNo ratings yet
- How To Stop Lying To Ourselves: A Call For Self-Awareness: REYNA, Kristinelou Marie N. STEM II - MendeleevDocument15 pagesHow To Stop Lying To Ourselves: A Call For Self-Awareness: REYNA, Kristinelou Marie N. STEM II - MendeleevRosemarie R. ReyesNo ratings yet
- [English] After Watching This, Your Brain Will Not Be the Same _ Lara Boyd _ TEDxVancouver [DownSub.com] (1)Document12 pages[English] After Watching This, Your Brain Will Not Be the Same _ Lara Boyd _ TEDxVancouver [DownSub.com] (1)Maulana Yazid Al AnnuriNo ratings yet
- (General Pathology) - (Wound Healing) by (Dr. Craig)Document24 pages(General Pathology) - (Wound Healing) by (Dr. Craig)NYUCD17No ratings yet
- Special Report: New Treatment For People With Dizziness and Balance Disorders by Dr. Keith LynchDocument9 pagesSpecial Report: New Treatment For People With Dizziness and Balance Disorders by Dr. Keith LynchlynchchiropracticNo ratings yet
- July Fibromyalgia Newsletter 2Document4 pagesJuly Fibromyalgia Newsletter 2JodieLynNo ratings yet
- Research Essay Final Draft - May 1-Avery CentersDocument13 pagesResearch Essay Final Draft - May 1-Avery Centersapi-609271780No ratings yet
- KNH 413 Case Study 4Document12 pagesKNH 413 Case Study 4api-272540385100% (1)
- Fall Newsletter Nov 14Document1 pageFall Newsletter Nov 14NYUCD17No ratings yet
- Reminders:: T Shirt Design Contes T!Document1 pageReminders:: T Shirt Design Contes T!NYUCD17No ratings yet
- Happy: TurkeyDocument8 pagesHappy: TurkeyNYUCD17No ratings yet
- Week of October 26th, 2015 - Class of 2017 NewsletterDocument9 pagesWeek of October 26th, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of September 5Document1 pageWeek of September 5NYUCD17No ratings yet
- Week of November 30th, 2015 - Class of 2017 NewsletterDocument9 pagesWeek of November 30th, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Fall Newsletter #3Document1 pageFall Newsletter #3NYUCD17No ratings yet
- Week of September 12Document1 pageWeek of September 12NYUCD17No ratings yet
- Happy: TurkeyDocument8 pagesHappy: TurkeyNYUCD17No ratings yet
- Week of November 2nd, 2015 - Class of 2017 NewsletterDocument10 pagesWeek of November 2nd, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of November 9th, 2015 - Class of 2017 NewsletterDocument9 pagesWeek of November 9th, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of October 5th, 2015 - Class of 2017 NewsletterDocument8 pagesWeek of October 5th, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of October 19th, 2015 - Class of 2017 NewsletterDocument9 pagesWeek of October 19th, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of September 14, 2015 - Class of 2017 NewsletterDocument7 pagesWeek of September 14, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of September 28, 2015 - Class of 2017 NewsletterDocument8 pagesWeek of September 28, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of September 21st, 2015 - Class of 2017 NewsletterDocument8 pagesWeek of September 21st, 2015 - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of September 8th - Class of 2017 NewsletterDocument8 pagesWeek of September 8th - Class of 2017 NewsletterNYUCD17No ratings yet
- Week of September 8th - Class of 2017 NewsletterDocument8 pagesWeek of September 8th - Class of 2017 NewsletterNYUCD17No ratings yet
- September 2, 2015 MinutesDocument3 pagesSeptember 2, 2015 MinutesNYUCD17No ratings yet
- Week of August 31st - Class of 2017 NewsletterDocument7 pagesWeek of August 31st - Class of 2017 NewsletterNYUCD17No ratings yet
- 10-17-14 MinutesDocument2 pages10-17-14 MinutesNYUCD17No ratings yet
- Week of August 31st - Class of 2017 NewsletterDocument7 pagesWeek of August 31st - Class of 2017 NewsletterNYUCD17No ratings yet
- July 8, 2015 Meeting MinutesDocument2 pagesJuly 8, 2015 Meeting MinutesNYUCD17No ratings yet
- 1-23-15 MinutesDocument2 pages1-23-15 MinutesNYUCD17No ratings yet
- September 2, 2015 MinutesDocument3 pagesSeptember 2, 2015 MinutesNYUCD17No ratings yet
- D2 Council Meeting Minutes: 12:00 - 1:00pm Room 8SDocument3 pagesD2 Council Meeting Minutes: 12:00 - 1:00pm Room 8SNYUCD17No ratings yet
- 2-20-15 MinutesDocument2 pages2-20-15 MinutesNYUCD17No ratings yet
- 1-9-15 MinutesDocument3 pages1-9-15 MinutesNYUCD17No ratings yet
- Effect of Oncoxin Oral Solution in HER2-Overexpressing Breast CancerDocument12 pagesEffect of Oncoxin Oral Solution in HER2-Overexpressing Breast Cancerleonaldy sintesahealthNo ratings yet
- Anil Kumar (Cell Biology) - 1Document11 pagesAnil Kumar (Cell Biology) - 1BISWANATH ROUTNo ratings yet
- FCVM 09 875434Document16 pagesFCVM 09 875434Sebastian WallotNo ratings yet
- Types of Cell Death: Apoptosis, Necrosis and AutophagyDocument10 pagesTypes of Cell Death: Apoptosis, Necrosis and AutophagyShreya NandyNo ratings yet
- Abhrak Bhasma (Biotite Mica Nanoparticles) Induces Cytotoxicity in Adenocarcinoma Human Alveolar Basal Epithelial Cells (A549)Document6 pagesAbhrak Bhasma (Biotite Mica Nanoparticles) Induces Cytotoxicity in Adenocarcinoma Human Alveolar Basal Epithelial Cells (A549)International Journal of Innovative Science and Research Technology100% (1)
- Nobel Prize winning research on programmed cell deathDocument1 pageNobel Prize winning research on programmed cell deathArgo DalapatiNo ratings yet
- Aids 2013Document404 pagesAids 2013kovaron80No ratings yet
- Apoptosis en Tejidos OralesDocument4 pagesApoptosis en Tejidos Oralesangie catalina estupiñan mirandaNo ratings yet
- CellDocument14 pagesCellSyrian AsadNo ratings yet
- Topic 1 and Topic 6Document71 pagesTopic 1 and Topic 6Majd MerieNo ratings yet
- Pentapods Products - Your Delicious Future 2300ADDocument4 pagesPentapods Products - Your Delicious Future 2300ADrutiusNo ratings yet
- S807 Mini Review v4Document37 pagesS807 Mini Review v4Daen de LeonNo ratings yet
- Ehac 604Document13 pagesEhac 604Edward ElBuenoNo ratings yet
- tmpD824 TMPDocument12 pagestmpD824 TMPFrontiersNo ratings yet
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- 01introduction To PathologyDocument71 pages01introduction To PathologyAishwarya PanchalNo ratings yet
- Cell DeathDocument21 pagesCell DeathBlaNo ratings yet
- Cluster of Differentiation Antigen PosterDocument1 pageCluster of Differentiation Antigen PosterReeti R. Bhat100% (1)
- Thesis Final 1Document40 pagesThesis Final 1John Paolo OcampoNo ratings yet
- Molecular Mechanism of Aloe Barbadensis MillerDocument8 pagesMolecular Mechanism of Aloe Barbadensis MillerSusyana IrianiNo ratings yet
- G0703017291 PDFDocument20 pagesG0703017291 PDFRed DiggerNo ratings yet
- Journal of Clinical and Experimental PharmacologyDocument13 pagesJournal of Clinical and Experimental PharmacologyCodruta Sandi100% (1)
- J Ournal J Ournal: Bioprocessing BioprocessingDocument10 pagesJ Ournal J Ournal: Bioprocessing BioprocessinghakancengizNo ratings yet
- REFERAT - Ppt.pathophysiology of PROM-noviDocument16 pagesREFERAT - Ppt.pathophysiology of PROM-noviFrisma Indah Permatasari100% (1)
- Nanocolloids For Nanomedicine and Drug DeliveryDocument274 pagesNanocolloids For Nanomedicine and Drug Deliveryenock-readersNo ratings yet
- Honey - The Natural Sweetener Become A PR PDFDocument13 pagesHoney - The Natural Sweetener Become A PR PDFLiyeta AlexinaNo ratings yet
- Franco 2017Document12 pagesFranco 2017ReshmaaRajendranNo ratings yet
- Role of Oxidative Stress in Semen Quality of Infertile MenDocument9 pagesRole of Oxidative Stress in Semen Quality of Infertile MenAyadPalaniNo ratings yet




















































![[English] After Watching This, Your Brain Will Not Be the Same _ Lara Boyd _ TEDxVancouver [DownSub.com] (1)](https://imgv2-1-f.scribdassets.com/img/document/720241560/149x198/bd20610543/1712300807?v=1)