Professional Documents
Culture Documents
Blunt Abdominal Trauma
Uploaded by
Den SinyoOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Blunt Abdominal Trauma
Uploaded by
Den SinyoCopyright:
Available Formats
Blunt Abdominal Trauma
Author: Eric L Legome, MD; Chief Editor: John Geibel, MD, DSc, MA
Updated: Mar 28, 2014
Overview
Practice Essentials
Blunt abdominal trauma is a leading cause of morbidity and mortality among all age groups. Identification of
serious intra-abdominal pathology is often challenging; many injuries may not manifest during the initial
assessment and treatment period.
Signs and symptoms
The initial clinical assessment of patients with blunt abdominal trauma is often difficult and notably
inaccurate. The most reliable signs and symptoms in alert patients are as follows:
Pain
Tenderness
Gastrointestinal hemorrhage
Hypovolemia
Evidence of peritoneal irritation
However, large amounts of blood can accumulate in the peritoneal and pelvic cavities without any significant
or early changes in the physical examination findings. Bradycardia may indicate the presence of free
intraperitoneal blood.
On physical examination, the following injury patterns predict the potential for intra-abdominal trauma:
Lap belt marks: Correlate with small intestine rupture
Steering wheelshaped contusions
Ecchymosis involving the flanks (Grey Turner sign) or the umbilicus (Cullen sign): Indicates
retroperitoneal hemorrhage, but is usually delayed for several hours to days
Abdominal distention
Auscultation of bowel sounds in the thorax: May indicate a diaphragmatic injury
Abdominal bruit: May indicate underlying vascular disease or traumatic arteriovenous fistula
Local or generalized tenderness, guarding, rigidity, or rebound tenderness: Suggests peritoneal injury
Fullness and doughy consistency on palpation: May indicate intra-abdominal hemorrhage
Crepitation or instability of the lower thoracic cage: Indicates the potential for splenic or hepatic injuries
See Clinical Presentation for more detail.
Diagnosis
Assessment of hemodynamic stability is the most important initial concern in the evaluation of a patient with
blunt abdominal trauma. In the hemodynamically unstable patient, a rapid evaluation for hemoperitoneum
can be accomplished by means of diagnostic peritoneal lavage (DPL) or the focused assessment with
sonography for trauma (FAST). Radiographic studies of the abdomen are indicated in stable patients when
the physical examination findings are inconclusive.
Diagnostic peritoneal lavage
DPL is indicated for the following patients in the setting of blunt trauma:
Patients with a spinal cord injury
Those with multiple injuries and unexplained shock
Obtunded patients with a possible abdominal injury
Intoxicated patients in whom abdominal injury is suggested
Patients with potential intra-abdominal injury who will undergo prolonged anesthesia for another
procedure
FAST
Bedside ultrasonography is a rapid, portable, noninvasive, and accurate examination that can be performed
by emergency clinicians and trauma surgeons to detect hemoperitoneum.
The current FAST examination protocol consists of 4 acoustic windows (pericardiac, perihepatic, perisplenic,
pelvic) with the patient supine.
An examination is interpreted as positive if free fluid is found in any of the 4 acoustic windows, negative if no
fluid is seen, and indeterminate if any of the windows cannot be adequately assessed.
Computed tomography
Computed tomography is the standard for detecting solid organ injuries. CT scans provide excellent imaging
of the pancreas, duodenum, and genitourinary system.
CT scanning often provides the most detailed images of traumatic pathology and may assist in determination
of operative intervention
[1, 2, 3, 4]
Unlike DPL or FAST, CT can determine the source of hemorrhage.
See Workup for more detail.
Management
Treatment of blunt abdominal trauma begins at the scene of the injury and is continued upon the patients
arrival at the ED or trauma center. Management may involve nonoperative measures or surgical treatment,
as appropriate.
Indications for laparotomy in a patient with blunt abdominal injury include the following:
Signs of peritonitis
Uncontrolled shock or hemorrhage
Clinical deterioration during observation
Hemoperitoneum findings on FAST or DPL
Nonoperative management
In blunt abdominal trauma, including severe solid organ injuries, selective nonoperative management has
become the standard of care. Nonoperative management strategies are based on CT scan diagnosis and
the hemodynamic stability of the patient, as follows:
For the most part, pediatric patients can be resuscitated and treated nonoperatively; some pediatric
surgeons often transfuse up to 40 mL/kg of blood products in an effort to stabilize a pediatric patient
Hemodynamically stable adults with solid organ injuries, primarily those to the liver and spleen, may be
candidates for nonoperative management
Splenic artery embolotherapy, although not standard of care, may be used for adult blunt splenic injury
Nonoperative management involves closely monitoring vital signs and frequently repeating the physical
examination
See Treatment and Medication for more detail.
Image library
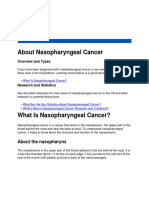
Blunt abdominal trauma. Right kidney injury with blood in perirenal space. Injury resulted from high-speed motor vehicle collision
Pathophysiology
Intra-abdominal injuries secondary to blunt force are attributed to collisions between the injured person and
the external environment and to acceleration or deceleration forces acting on the persons internal organs.
Blunt force injuries to the abdomen can generally be explained by 3 mechanisms.
The first mechanism is deceleration. Rapid deceleration causes differential movement among adjacent
structures. As a result, shear forces are created and cause hollow, solid, visceral organs and vascular
pedicles to tear, especially at relatively fixed points of attachment. For example, the distal aorta is attached to
the thoracic spine and decelerates much more quickly than the relatively mobile aortic arch. As a result,
shear forces in the aorta may cause it to rupture. Similar situations can occur at the renal pedicles and at the
cervicothoracic junction of the spinal cord.
Classic deceleration injuries include hepatic tear along the ligamentum teres and intimal injuries to the renal
arteries. As bowel loops travel from their mesenteric attachments, thrombosis and mesenteric tears, with
resultant splanchnic vessel injuries, can result.
The second mechanism involves crushing. Intra-abdominal contents are crushed between the anterior
abdominal wall and the vertebral column or posterior thoracic cage. This produces a crushing effect, to which
solid viscera (eg, spleen, liver, kidneys) are especially vulnerable.
The third mechanism is external compression, whether from direct blows or from external compression
against a fixed object (eg, lap belt, spinal column). External compressive forces result in a sudden and
dramatic rise in intra-abdominal pressure and culminate in rupture of a hollow viscous organ (ie, in
accordance with the principles of Boyle law).
The liver and spleen seem to be the most frequently injured organs, though reports vary. The small and large
intestines are the next most frequently injured organs. Recent studies show an increased number of hepatic
injuries, perhaps reflecting increased use of CT scanning and concomitant identification of more injuries.
Etiology
Vehicular trauma is by far the leading cause of blunt abdominal trauma in the civilian population. Auto-to-
auto and auto-to-pedestrian collisions have been cited as causes in 50-75% of cases. Other common
etiologies include falls and industrial or recreational accidents. Rare causes of blunt abdominal injuries
include iatrogenic trauma during cardiopulmonary resuscitation, manual thrusts to clear an airway, and the
Heimlich maneuver.
Background
The care of the trauma patient is demanding and requires speed and efficiency. Evaluating patients who
have sustained blunt abdominal trauma remains one of the most challenging and resource-intensive aspects
of acute trauma care.
[5, 6]
Blunt abdominal trauma is a leading cause of morbidity and mortality among all age groups. Identification of
serious intra-abdominal pathology is often challenging. Many injuries may not manifest during the initial
assessment and treatment period. Missed intra-abdominal injuries and concealed hemorrhage are frequent
causes of increased morbidity and mortality, especially in patients who survive the initial phase after an
injury.
Physical examination findings are notoriously unreliable. One reason is that mechanisms of injury often result
in other associated injuries that may divert the physicians attention from potentially life-threatening intra-
abdominal pathology. Other common reasons are an altered mental state and drug and alcohol intoxication.
Coordinating a trauma resuscitation demands a thorough understanding of the pathophysiology of trauma
and shock, excellent clinical and diagnostic acumen, skill with complex procedures, compassion, and the
ability to think rationally in a chaotic milieu.
Blunt abdominal trauma usually results from motor vehicle collisions (MVCs), assaults, recreational
accidents, or falls. The most commonly injured organs are the spleen, liver, retroperitoneum, small bowel,
kidneys (see the image below), bladder, colorectum, diaphragm, and pancreas. Men tend to be affected
slightly more often than women.
Blunt abdominal trauma. Right kidney injury with blood in perirenal space. Injury resulted from high-speed motor vehicle collision
For more information, see the following:
Pediatric Abdominal Trauma
Penetrating Abdominal Trauma
Focused Assessment with Sonography in Trauma (FAST)
Abdominal Vascular Injuries
Anatomy
The abdomen can be arbitrarily divided into 4 areas. The first is the intrathoracic abdomen, which is the
portion of the upper abdomen that lies beneath the rib cage. Its contents include the diaphragm, liver,
spleen, and stomach. The rib cage makes this area inaccessible to palpation and complete examination.
The second is the pelvic abdomen, which is defined by the bony pelvis. Its contents include the urinary
bladder, urethra, rectum, small intestine, and, in females, ovaries, fallopian tubes, and uterus. Injury to these
structures may be extraperitoneal in nature and therefore difficult to diagnose.
The third is the retroperitoneal abdomen, which contains the kidneys, ureters, pancreas, aorta, and vena
cava. Injuries to these structures are very difficult to diagnose on the basis of physical examination findings.
Evaluation of the structures in this region may require computed tomography (CT) scanning, angiography,
and intravenous pyelography (IVP).
The fourth is the true abdomen, which contains the small and large intestines, the uterus (if gravid), and the
bladder (when distended). Perforation of these organs is associated with significant physical findings and
usually manifests with pain and tenderness from peritonitis. Plain x-ray films are helpful if free air is present.
Additionally, diagnostic peritoneal lavage (DPL) is a useful adjunct.
Epidemiology
United States statistics
By nearly every measure, injury ranks as one of the most pressing health issues in the United States. More
than 150,000 people die each year as a result of injuries, such as motor vehicle crashes, fires, falls,
drowning, poisoning, suicide, and homicide. Injuries are the leading cause of death and disability for US
children and young adults.
According to the 2000 statistics from the National Center for Injury Prevention and Control, trauma
(unintentional and intentional) was the leading cause of death in persons aged 1-44 years. Further review of
the data reveals that in those aged 15-25 years, 14,113 persons died from unintentional injuries, 73% of
which were related to vehicular trauma. In individuals aged 25-34 years, 57% of the 11,769 deaths reported
were from motor vehicle collisions.
In 2001, approximately 30 million people visited emergency departments (EDs) for the treatment of nonfatal
injuries, and more than 72,000 people were disabled by injuries. Injury imposes exceptional costs, both in
health care dollars and in human losses, to society.
The true frequency of blunt abdominal trauma, however, is unknown. Data collected from trauma centers
reflect patients who are transported to or seek care at these centers; these data may not reflect patients
presenting to other facilities. The incidence of out-of-hospital deaths is unknown.
One review from the National Pediatric Trauma Registry by Cooper et al reported that 8% of patients
(total=25,301) had abdominal injuries. Eighty-three percent of those injuries were from blunt mechanisms.
Automobile-related injuries accounted for 59% of those injuries.
[7]
Similar reviews from adult trauma
databases reflect that blunt trauma is the leading cause of intra-abdominal injury and that MVC is the leading
mode of injury. Blunt injuries account for approximately two thirds of all injuries.
Hollow viscus trauma is more frequent in the presence of an associated, severe, solid organ injury,
particularly to the pancreas. Approximately two thirds of patients with hollow viscus trauma are injured in
MVCs.
International statistics
In 1990, approximately 5 million people died worldwide as a result of injury. The risk of death from injury
varied strongly by region, age, and sex. Approximately 2 male deaths due to violence were reported for
every female death. Injuries accounted for approximately 12.5% of all male deaths, compared with 7.4% of
female deaths.
Globally, injury accounts for 10% of all deaths; however, injuries in sub-Saharan Africa are far more
destructive than in other areas. In sub-Saharan Africa, the risk of death from trauma is highest in those aged
15-60 years, and the proportion of such deaths from trauma is higher than in any other region of the world.
South Africa, for instance, has a traffic death rate per unit of distance traveled that is surpassed only by
those of Korea, Kenya, and Morocco.
Estimates indicate that by 2020, 8.4 million people will die yearly from injury, and injuries from traffic
collisions will be the third most common cause of disability worldwide and the second most common cause in
the developing world.
Data from the World Health Organization (WHO) indicate that falls from heights of less than 5 meters are the
leading cause of injury, and automobile crashes are the next most frequent cause. These data reflect all
injuries, not just blunt injuries to the abdomen.
A review from Singapore described trauma as the leading cause of death in those aged 1-44 years. Traffic
accidents, stab wounds, and falls from heights were the leading modes of injury. Blunt abdominal trauma
accounted for 79% of cases.
[8]
A similar paper from India reported that blunt abdominal trauma is more frequent in males aged 21-30 years;
the majority of patients were injured in automobile accidents. A German study indicated that, of patients with
vertical deceleration injuries (ie, falls from heights), only 5.9% had blunt abdominal injuries.
Age-related differences in incidence
Most studies indicate that the peak incidence is in persons aged 14-30 years. A review of 19,261 patients
with blunt abdominal trauma revealed equal incidence of hollow viscus injuries in both children (ie, 14 y)
and adults.
Sex-related differences in incidence
According to national and international data, blunt abdominal trauma is more common in men. The male-to-
female ratio is 60:40.
Prognosis
Overall prognosis for patients who sustain blunt abdominal trauma is favorable. Without statistics that
indicate the number of out-of-hospital deaths and the total number of patients with blunt trauma to the
abdomen, a description of the specific prognosis for patients with intra-abdominal injuries is difficult. Mortality
rates for hospitalized patients are approximately 5-10%.
The National Pediatric Trauma Registry reported that 9% of pediatric patients with blunt abdominal trauma
died. Of these, only 22% were reported as having intra-abdominal injuries as the likely cause of death.
[7]
A review from Australia of intestinal injuries in blunt trauma reported that 85% of injuries occurred from
vehicular accidents. The mortality rate was 6%. In a large review of operating room deaths in which blunt
trauma accounted for 61% of all injuries, abdominal trauma was the primary identified cause of death in
53.4% of cases.
Patient Education
Proper adjustment of restraints in motor vehicles is an important aspect of patient education. The following
are key recommendations:
Wear lap belts in conjunction with shoulder restraints.
Adjust lap belts so that they fit snugly, and place them across the lower abdomen and below the iliac
crests.
Wear restraints even in vehicles equipped with supplemental vehicle restraints (eg, airbags).
Adjust seats and steering wheels so that the distance between the abdominal wall and the steering
wheel is as wide as possible while still allowing proper control of the vehicle.
Advise patients to practice defensive driving by observing speed limits and keeping a safe distance between
them and other automobiles on the road.
For patient education resources, see the Kidneys and Urinary System Center, as well as Blood in the
Urine and Bruises.
Blunt Abdominal Trauma Clinical Presentation
History
Initially, evaluation and resuscitation of a trauma patient occur simultaneously. In general, do not obtain a
detailed history until life-threatening injuries have been identified and therapy has been initiated. The initial
assessment begins at the scene of the injury, with information provided by the patient, family, bystanders, or
paramedics, or police.
Important factors relevant to the care of a patient with blunt abdominal trauma, specifically those involving
motor vehicles, include the following:
The extent of vehicular damage
Whether prolonged extrication was required
Whether the passenger space was intruded
Whether a passenger died
Whether the person was ejected from the vehicle
The role of safety devices such as seat belts and airbags
The presence of alcohol or drug use
The presence of a head or spinal cord injury
Whether psychiatric problems were evident
Important elements of the pertinent history include the following:
Allergies
Medications
Past medical and surgical history
Time of last meal
Immunization status
Events leading to the incident
Social history, including history of substance abuse
Information from family and friends
The mnemonic AMPLE (A llergies, M edications, P ast medical history, L ast meal or other intake,
and E vents leading to presentation) is often useful as a means of remembering key elements of the history.
A history of out-of-hospital hypotension is a predictor of more significant intra-abdominal injuries. Even if the
patient is normotensive at arrival in the emergency department (ED), he or she should be considered to be at
increased risk.
Physical Examination
Primary survey
Resuscitation is performed concomitantly and continues as the physical examination is completed. Priorities
in resuscitation and diagnosis are established on the basis of hemodynamic stability and the degree of injury.
The goal of the primary survey, as directed by the Advanced Trauma Life Support (ATLS) protocol, is to
identify and expediently treat life-threatening injuries. The protocol includes the following:
Airway, with cervical spine precautions
Breathing
Circulation
Disability
Exposure
It is imperative for all personnel involved in the direct care of a trauma patient to exercise universal
precautions against body fluid exposure. The incidence of infectious diseases (eg, HIV, hepatitis) is
significantly higher in trauma patients than in the general public, with some centers reporting rates as high as
19%. Even in medical centers with relatively low rates of communicable diseases, safely determining who is
infected with such pathogens is impossible.
The standard barrier precautions include a hat, eye shield, face mask, gown, gloves, and shoe covers.
Unannounced trauma arrival is probably the most common situation that leads to a breach in barrier
precautions. Personnel must be instructed to adhere to these guidelines at all times, even if it means a 30-
second delay in patient care.
Secondary survey
After an appropriate primary survey and initiation of resuscitation, attention should be focused on the
secondary survey of the abdomen. The secondary survey is the identification of all injuries via a head-to-toe
examination. For life-threatening injuries that necessitate emergency surgery, a comprehensive secondary
survey should be delayed until the patient has been stabilized.
At the other end of the spectrum are victims of blunt trauma who have a benign abdomen upon initial
presentation. Many injuries initially are occult and manifest over time. Frequent serial examinations, in
conjunction with the appropriate diagnostic studies, such as abdominal computed tomography (CT) and
bedside ultrasonography, are essential in any patient with a significant mechanism of injury.
The evaluation of a patient with blunt abdominal trauma must be accomplished with the entire patient in
mind, with all injuries prioritized accordingly. This implies that injuries involving the head, the respiratory
system, or the cardiovascular system may take precedence over an abdominal injury.
The abdomen should neither be ignored nor be the sole focus of the treating clinician and surgeon. In an
unstable patient, the question of abdominal involvement must be expediently addressed. This is
accomplished by identifying free intra-abdominal fluid with diagnostic peritoneal lavage (DPL) or focused
assessment with sonography for trauma (FAST). The objective is rapid identification of those patients who
need a laparotomy.
The initial clinical assessment of patients with blunt abdominal trauma is often difficult and notably
inaccurate. Associated injuries often cause tenderness and spasms in the abdominal wall and make
diagnosis difficult. Lower rib fractures, pelvic fractures, and abdominal wall contusions may mimic the signs
of peritonitis. In a collected series of 955 patients, Powell et al reported that clinical evaluation alone has an
accuracy rate of only 65% for detecting the presence or absence of intraperitoneal blood.
[9]
In general, accuracy increases if the patient is reevaluated repeatedly and at frequent intervals. However,
repeated examinations may not be feasible in patients who need general anesthesia and surgery for other
injuries. The greatest compromise of the physical examination occurs in the setting of neurologic dysfunction,
which may be caused by head injury or substance abuse.
The most reliable signs and symptoms in alert patients are pain, tenderness, gastrointestinal hemorrhage,
hypovolemia, and evidence of peritoneal irritation. However, large amounts of blood can accumulate in the
peritoneal and pelvic cavities without any significant or early changes in the physical examination findings.
Bradycardia may indicate the presence of free intraperitoneal blood in a patient with blunt abdominal injuries.
The respiratory pattern should be observed because abdominal breathing may indicate spinal cord injury. A
sensory examination of the chest and abdomen should be performed to evaluate the potential for spinal cord
injury. Spinal cord injury may interfere with the accurate assessment of the abdomen by causing decreased
or absent pain perception.
The abdominal examination must be systematic. The abdomen is inspected for abrasions or ecchymosis.
Particular attention should be paid to injury patterns that predict the potential for intra-abdominal trauma (eg,
lap belt abrasions, steering wheelshaped contusions). In most studies, lap belt marks have been correlated
with rupture of the small intestine and an increased incidence of other intra-abdominal injuries.
Ecchymosis involving the flanks (Grey Turner sign) or the umbilicus (Cullen sign) indicates retroperitoneal
hemorrhage, but this is usually delayed for several hours to days.
Visual inspection for abdominal distention, which may be due to pneumoperitoneum, gastric dilatation
secondary to assisted ventilation or swallowing of air, or ileus produced by peritoneal irritation, is important.
Auscultation of bowel sounds in the thorax may indicate the presence of a diaphragmatic injury. Abdominal
bruit may indicate underlying vascular disease or traumatic arteriovenous fistula.
Palpation may reveal local or generalized tenderness, guarding, rigidity, or rebound tenderness, which
suggests peritoneal injury. Such signs appearing soon after an injury suggest leakage of intestinal content.
Peritonitis due to intra-abdominal hemorrhage may take several hours to develop.
Fullness and doughy consistency on palpation may indicate intra-abdominal hemorrhage. Crepitation or
instability of the lower thoracic cage indicates the potential for splenic or hepatic injuries associated with
lower rib injuries.
Tenderness on percussion constitutes a peritoneal sign. Tenderness mandates further evaluation and
probably surgical consultation.
Rectal and bimanual vaginal pelvic examinations should be performed.
[10]
A rectal examination should be
done to search for evidence of bony penetration resulting from a pelvic fracture, and the stool should be
evaluated for gross or occult blood. The evaluation of rectal tone is important for determining the patients
neurologic status, and palpation of a high-riding prostate suggests urethral injury.
The genitals and perineum should be examined for soft tissue injuries, bleeding, and hematoma. Pelvic
instability indicates the potential for lower urinary tract injury, as well as pelvic and retroperitoneal hematoma.
Open pelvic fractures are associated with a mortality rate exceeding 50%.
A nasogastric tube should be placed routinely (in the absence of contraindications, eg, basilar skull fracture)
to decompress the stomach and to assess for the presence of blood. If the patient has evidence of a
maxillofacial injury, an orogastric tube is preferred.
As the assessment continues, a Foley catheter is placed and a sample of urine is sent for analysis for
microscopic hematuria. If injury to the urethra or bladder is suggested because of an associated pelvic
fracture, then a retrograde urethrogram is performed before catheterization.
With respect to the primary and secondary surveys, pediatric patients are assessed and treatedat least
initiallyas adults. However, there are obvious anatomic and clinical differences between children and
adults that must be kept in mind, including the following:
A pediatric patients physiologic response to injury is different.
Effective communication with a child is not always possible.
Physical examination findings become more important in children.
A pediatric patients blood volume is smaller, predisposing to rapid exsanguinations.
Technical procedures in pediatric patients tend to be more time consuming and challenging.
A childs relatively large body surface area contributes to rapid heat loss.
Perhaps the most significant difference between pediatric and adult blunt trauma is that, for the most part,
pediatric patients can be resuscitated and treated nonoperatively. Some pediatric surgeons often transfuse
up to 40 mL/kg of blood products in an effort to stabilize a pediatric patient. Obviously, if this fails and the
child continues to be unstable, laparotomy is indicated.
Tertiary survey
The concept of the tertiary trauma survey was first introduced by Enderson et al to assist in the diagnosis of
any injuries that may have been missed during the primary and secondary surveys.
[11]
The tertiary survey
involves a repetition of the primary and secondary surveys and a revision of all laboratory and radiographic
studies. In 1 study, a tertiary trauma survey detected 56% of injuries missed during the initial assessment
within 24 hours of admission.
[12]
Blunt Abdominal Trauma Differential Diagnoses
Diagnostic Considerations
Identification of intra-abdominal injuries can be challenging. Common pitfalls in diagnosis include the
following:
Failure to suspect intra-abdominal injury from appropriate mechanisms
Failure to evaluate abdominal/flank/costal margin pain after blunt abdominal injury
Failure to obtain timely surgical consultation and operative intervention
Failure to recognize intra-abdominal hemorrhage and delay operation for additional diagnostic testing in
the face of hemodynamic compromise
Differential Diagnoses
Domestic Violence
Hemorrhagic Stroke
Hypovolemic Shock
Lower Genitourinary Trauma
Penetrating Abdominal Trauma in Emergency Medicine
Pregnancy Trauma
Upper Genitourinary Trauma
Blunt Abdominal Trauma Workup
Approach Considerations
In recent years, laboratory evaluation of trauma patients has been a matter of significant discussion.
Commonly recommended studies include serum glucose, complete blood count (CBC), serum chemistries,
serum amylase, urinalysis, coagulation studies, blood typing and cross-matching, arterial blood gases
(ABGs), blood ethanol, urine drug screens, and a urine pregnancy test (for females of childbearing age).
Serum electrolyte values, creatinine level, and glucose values are often obtained for reference, but typically
they have little or no value in the initial management period.
Aggressive radiographic and surgical investigation is indicated in patients with persistent hyperamylasemia
or hyperlipasemia, conditions that suggest significant intra-abdominal injury.
All patients should have their tetanus immunization history reviewed. If it is not current, prophylaxis should be
given.
The most important initial concern in the evaluation of a patient with blunt abdominal trauma is an
assessment of hemodynamic stability. In the hemodynamically unstable patient, a rapid evaluation must be
made regarding the presence of hemoperitoneum. This can be accomplished by means of diagnostic
peritoneal lavage (DPL) or the focused assessment with sonography for trauma (FAST). Radiographic
studies of the abdomen are indicated in stable patients when the physical examination findings are
inconclusive.
Go to Focused Assessment with Sonography in Trauma (FAST) for complete information on this topic.
Blood Studies
Complete blood count
The presence of massive hemorrhage is usually obvious from hemodynamic parameters, and an abnormal
hematocrit value merely confirms the diagnosis. Normal hemoglobin and hematocrit results do not rule out
significant hemorrhage. Patients bleed whole blood. Until blood volume is replaced with crystalloid solution or
hormonal effects (eg, adrenocorticotropic hormone [ACTH], aldosterone, antidiuretic hormone [ADH]) and
transcapillary refill occurs, anemia may not develop.
Bedside diagnostic testing with rapid hemoglobin or hematocrit machines may quickly identify patients who
have physiologically significant volume deficits and hemodilution. Reported hemoglobin from ABG
measurements also may be useful in identifying anemia. Some studies have correlated a low initial
hematocrit (ie, < 30%) with significant injuries.
Do not withhold transfusion in patients who have relatively normal hematocrit results (ie, >30%) but have
evidence of clinical shock, serious injuries (eg, open-book pelvic fracture), or significant ongoing blood loss.
Hemodynamic instability in an adult despite the administration of 2 L of fluid indicates ongoing blood loss and
is an indication for immediate blood transfusion. Use platelet transfusions to treat patients with
thrombocytopenia (ie, platelet count < 50,000/L) and ongoing hemorrhage.
An elevated white blood cell (WBC) count on admission is nonspecific and does not predict the presence of a
hollow viscus injury (HVI). The diagnostic value of serial WBC counts for predicting HVI within the first 24
hours after trauma is very limited.
[13]
Serum electrolyte measurements
Recently, the usefulness of routine serum chemistries of trauma patients has been questioned. Most trauma
victims are younger than 40 years and rarely are taking medications that may alter electrolytes (eg, diuretics,
potassium replacements).
The more prudent choice when attempting to limit cost involves selective ordering of these studies. Selection
should be based on the patients medications, the presence of concurrent nausea or vomiting, the presence
of dysrhythmias, or a history of renal failure or other chronic medical problems associated with electrolyte
imbalance.
Serum glucose and carbon dioxide measurements
If blood gas measurements are not routinely obtained, serum chemistries that measure serum glucose and
carbon dioxide levels are indicated. Rapid bedside blood-glucose determination, obtained with a finger-stick
measuring device, is important for patients with altered mental status.
Liver function tests
Liver function tests (LFTs) may be useful in the patient with blunt abdominal trauma; however, test findings
may be elevated for several reasons (eg, alcohol abuse).
[14]
One study has shown that an aspartate
aminotransferase (AST) or alanine aminotransferase (ALT) level more than 130 U corresponds with
significant hepatic injury.
[15]
Lactate dehydrogenase (LDH) and bilirubin levels are not specific indicators of
hepatic trauma.
Serum amylase or lipase measurements
The serum lipase or amylase level is neither sensitive nor specific as a marker for major pancreatic or enteric
injury. Normal levels do not exclude a major pancreatic injury. Elevated levels may be caused by injuries to
the head and face or by an assortment of nontraumatic causes (eg, alcohol, narcotics, various other drugs).
Amylase or lipase levels may be elevated because of pancreatic ischemia caused by the systemic
hypotension that accompanies trauma.
However, persistent hyperamylasemia or hyperlipasemia (eg, abnormal elevation 3-6 hours after trauma)
should raise the suggestion of significant intra-abdominal injury and is an indication for aggressive
radiographic and surgical investigation.
Coagulation profile
The cost-effectiveness of routine prothrombin time (PT)/activated partial thromboplastin time (aPTT)
determination upon admission is questionable. PT or aPTT should be measured in patients who have a
history of blood dyscrasias (eg, hemophilia), who have synthetic problems (eg, cirrhosis), or who take
anticoagulant medications (eg, warfarin, heparin).
Blood typing, screening, and cross-matching
Blood from all trauma patients with suspected blunt abdominal injury should be screened and typed. If an
injury is identified, this practice greatly reduces the time required for cross-matching. An initial cross-match
should be performed on a minimum of 4-6 units for those patients with clear evidence of abdominal injury
and hemodynamic instability. Until cross-matched blood is available, O-negative or type-specific blood
should be used.
Arterial blood gas measurements
ABG values may provide important information in major trauma victims. In addition to information about
oxygenation (eg, partial pressure of oxygen [PO2] and arterial oxygen saturation [SaO2]) and ventilation
(partial pressure of carbon dioxide [PCO2]), this test provides valuable information regarding oxygen delivery
through calculation of the alveolar-arterial (A-a) gradient. ABG determinations also report total hemoglobin
more rapidly than CBCs.
Upon initial hospital admission, suspect metabolic acidemia to result from the lactic acidosis that
accompanies shock. A moderate base deficit (ie, more than 5 mEq) indicates the need for aggressive
resuscitation and determination of the etiology.
Attempt to improve systemic oxygen delivery by ensuring an adequate SaO2 (ie, >90%) and by acquiring
volume resuscitation with crystalloid solutions and, if indicated, blood.
Drug and alcohol screening
Perform drug and alcohol screens on trauma patients who have alterations in their level of consciousness.
Breath or blood testing may quantify alcohol level.
Urine Studies
Indications for diagnostic urinalysis include significant trauma to the abdomen and/or flank, gross hematuria,
microscopic hematuria in the setting of hypotension, and a significant deceleration mechanism.
[16]
Obtain a contrast nephrogram by utilizing intravenous pyelography (IVP) or computed tomography (CT)
scanning with intravenous (IV) contrast. Gross hematuria indicates a workup that includes cystography and
IVP or CT scanning of the abdomen with contrast.
Perform a urine toxicologic screen as appropriate. Obtain a serum or urine pregnancy test on all females of
childbearing age.
Plain Radiography
Although their overall value in the evaluation of patients with blunt abdominal trauma is limited, plain films
can demonstrate numerous findings. The chest radiograph may aid in the diagnosis of abdominal injuries
such as ruptured hemidiaphragm (eg, a nasogastric tube seen in the chest) or pneumoperitoneum.
The pelvic or chest radiograph can demonstrate fractures of the thoracolumbar spine. The presence of
transverse fractures of the vertebral bodies (ie, Chance fractures) suggests a higher likelihood of blunt
injuries to the bowel. In addition, free intraperitoneal air, or trapped retroperitoneal air from duodenal
perforation, may be seen.
Ultrasonography
The use of diagnostic ultrasonography to evaluate a patient with blunt trauma for abdominal injuries has
been advocated since the 1970s. European and Asian investigators have extensive experience with this
technology and are leaders in the use of ultrasound for the diagnosis of blunt abdominal trauma.
The first American report of physician-performed abdominal ultrasonography in the evaluation of blunt
abdominal trauma was published in 1992 by Tso and colleagues.
[17]
Since then, numerous articles have been
published in the United States advocating the use of ultrasound (ie, FAST) in the evaluation of the patient
with blunt abdominal trauma.
Bedside ultrasonography is a rapid, portable, noninvasive, and accurate examination that can be performed
by emergency clinicians and trauma surgeons to detect hemoperitoneum. In fact, in many medical centers,
the FAST examination has virtually replaced DPL as the procedure of choice in the evaluation of
hemodynamically unstable trauma patients.
The FAST examination is based on the assumption that all clinically significant abdominal injuries are
associated with hemoperitoneum. However, the detection of free intraperitoneal fluid is based on factors
such as the body habitus, injury location, presence of clotted blood, position of the patient, and amount of
free fluid present.
In a patient with isolated blunt abdominal trauma and multisystem injuries, FAST performed by an
experienced sonographer can rapidly identify free intraperitoneal fluid (generally appearing as a black stripe).
The sensitivity for solid organ encapsulated injury is moderate in most studies. Hollow viscus injury (HVI)
rarely is identified; however, free fluid may be visualized. For patients with persistent pain or tenderness or
those developing peritoneal signs, FAST may be considered as a complementary measure to CT scanning,
DPL, or exploration.
The minimum threshold for detecting hemoperitoneum is unknown and remains a subject of interest.
Kawaguchi and colleagues found that 70 mL of blood could be detected,
[18]
whereas Tiling et al found that 30
mL is the minimum requirement for detection with ultrasonography.
[19]
They also concluded that a small
anechoic stripe in the Morison pouch represents approximately 250 mL of fluid, whereas 0.5-cm and 1-cm
stripes represent approximately 500 mL and 1 L of free fluid, respectively.
The current FAST examination protocol consists of 4 acoustic windows with the patient supine. These
windows are pericardiac, perihepatic, perisplenic, and pelvic (known as the 4 P s). An examination is
interpreted as positive if free fluid is found in any of the 4 acoustic windows and as negative if no fluid is
seen. An examination is deemed indeterminate if any of the windows cannot be adequately assessed.
The pericardial window is obtained via a subcostal or transthoracic approach. It provides a 4-chamber view
of the heart and can detect the presence of hemopericardium, which is demonstrated by the separation of
the visceral and parietal pericardial layers. The perihepatic window yields views of portions of the liver,
diaphragm, and right kidney. It reveals fluid in the Morison pouch (see the images below), the subphrenic
space, and the right pleural space.
Blunt abdominal trauma. Normal Morison pouch (ie, no free fluid).
Blunt abdominal trauma. Free fluid in Morison pouch
The perisplenic window provides views of the spleen and the left kidney and reveals fluid in the splenorenal
recess (see the images below), the left pleural space, and the subphrenic space. The pelvic window makes
use of the bladder as a sonographic window and thus is best accomplished while the patient has a full
bladder. In males, free fluid is seen as an anechoic area (sonographically black) in the rectovesicular pouch
or cephalad to the bladder. In females, fluid accumulates in the Douglas pouch, posterior to the uterus.
Blunt abdominal trauma. Normal splenorenal recess.
Blunt abdominal trauma. Free fluid in splenorenal recess.
FASTs diagnostic accuracy generally is equal to that of DPL. Studies in the United States have
demonstrated the value of bedside sonography as a noninvasive approach for rapid evaluation of
hemoperitoneum. The studies demonstrate a degree of operator dependence; however, some studies have
shown that with a structured learning session, even novice operators can identify free intra-abdominal fluid,
especially if more than 500 mL of fluid is present. Sensitivity and specificity of these studies range from 85%
to 95%.
[20, 21, 22, 23, 24]
As noted, FAST relies on hemoperitoneum to identify patients with injury. Chiu and colleagues, in their study
of 772 patients with blunt trauma undergoing FAST scans, reported 52 patients had an abdominal
injury.
[25]
Of the 52 patients, 15 (29%) had no hemoperitoneum on FAST or CT scan results. These findings
suggest that the reliance on hemoperitoneum as the sole indicator of abdominal visceral injury limits the
utility of FAST as a diagnostic screening tool in stable patients with blunt abdominal trauma.
Rozycki et al studied 1540 patients and reported that ultrasonography was the most sensitive and specific
modality for the evaluation of hypotensive patients with blunt abdominal trauma (sensitivity and specificity,
100%).
[24]
Hemodynamically stable patients with positive FAST results may require a CT scan to better define the
nature and extent of their injuries. Taking every patient with a positive FAST result to the operating room may
result in an unacceptably high laparotomy rate.
Hemodynamically stable patients with negative FAST results require close observation, serial abdominal
examinations, and a follow-up FAST examination. However, strongly consider performing a CT scan,
especially if the patient is intoxicated or has other associated injuries.
Hemodynamically unstable patients with negative FAST results are a diagnostic challenge. Options include
DPL, exploratory laparotomy, and, possibly, a CT scan after aggressive resuscitation.
Go to Focused Assessment with Sonography in Trauma (FAST) for complete information on this topic.
Computed Tomography
Although expensive and potentially time-consuming, CT scanning often provides the most detailed images of
traumatic pathology and may assist in determination of operative intervention.
[1, 2, 3, 4]
CT remains the criterion
standard for the detection of solid organ injuries (see the image below). In addition, a CT scan of the
abdomen can reveal other associated injuries, notably vertebral and pelvic fractures and injuries in the
thoracic cavity.
Blunt abdominal trauma with liver laceration.
CT scanning, unlike DPL or FAST, has the capability to determine the source of hemorrhage (see the image
below). In addition, many retroperitoneal injuries go unnoticed with DPL and FAST examinations.
Blunt abdominal trauma with splenic injury and hemoperitoneum.
Transport only hemodynamically stable patients to the CT scanner. When performing CT scans, closely and
carefully monitor vital signs for clinical evidence of decompensation. Preliminary evidence suggests that a
flat vena cava on CT scan is a marker for underresuscitation and may be correlated with higher mortality and
hemodynamic decompensation.
[26]
CT scans provide excellent imaging of the pancreas, duodenum, and genitourinary system. The images can
help quantitate the amount of blood in the abdomen and can reveal individual organs with precision. The
primary advantage of CT scanning is its high specificity and use for guiding nonoperative management of
solid organ injuries.
Drawbacks of CT scanning relate to the need to transport the patient from the trauma resuscitation area and
the additional time required to perform CT scanning compared to FAST or DPL.
In addition, CT scanning may miss injuries to the diaphragm and perforations of the gastrointestinal (GI)
tract, especially when performed soon after the injury. Although some pancreatic injuries may be missed with
a CT scan performed soon after trauma, virtually all are identified if the scan is repeated in 36-48 hours. For
selected patients, endoscopic retrograde cholangiopancreatography (ERCP) may complement CT scanning
to rule out a ductal injury.
Finally, CT scanning is relatively expensive and time consuming and requires oral or intravenous (IV)
contrast, which may cause adverse reactions. The best CT imagery requires both oral and IV contrast. Some
controversy has arisen over the use of oral contrast and whether the additional information it provides
negates the drawbacks of increased time to administration and risk of aspiration. The value of oral contrast in
diagnosing bowel injury has been debated, but no definitive answer exists at this time.
A prediction rule created by Holmes and colleagues for use in children who have suffered blunt torso trauma
demonstrated a negative predictive value of 99.9% for identifying patients at very low risk for intra-abdominal
injuries undergoing acute intervention and for whom CT scanning could be obviated.
[27]
The rule consists of
the following 7 patient history and physical examination findings (in descending order of importance):
No evidence of abdominal wall trauma or seat belt sign
Glasgow Coma Scale score >13 (see the Glasgow Coma Scale calculator)
No abdominal tenderness
No evidence of thoracic wall trauma
No complaints of abdominal pain
No decreased breath sounds
No vomiting
Diagnostic Laparoscopy
The introduction of minimally invasive surgery has revolutionized many surgical diagnostic protocols. In the
late 1980s and early 1990s, there was considerable interest in the use of laparoscopy for evaluation and
management of blunt and penetrating abdominal trauma. Subsequent studies, however, revealed major
limitations to this approach and cautioned against its widespread use. The most important limitation is
inability to reliably identify hollow viscus and retroperitoneal injuries, even in the hands of experienced
laparoscopists.
Diagnostic laparoscopy involves placing a subumbilical or subcostal trocar for the introduction of the
laparoscope and creating other ports for retractors, clamps, and other tools necessary for visualization of the
repair.
Diagnostic laparoscopy has been most useful in the evaluation of possible diaphragmatic injuries, especially
in penetrating thoracoabdominal injuries on the left side.
[28, 29, 30]
In blunt trauma, it has no clear advantages
over less invasive modalities such as DPL and CT scanning; furthermore, complications can result from
trocar misplacement.
Diagnostic Peritoneal Lavage
The idea of evaluating the abdomen by analyzing its contents was first used in the diagnosis of acute
abdominal conditions. In 1906, Salomon described the passage of a urethral catheter by means of a trocar
inserted through the abdominal wall to obtain samples of peritoneal fluid with the aim of establishing the
diagnosis of peritonitis from infectious agents (eg, pneumococcal or tuberculous organisms). This technique
has since been refined and is now known as abdominal paracentesis.
In 1926, Neuhof and Cohen described the sampling of peritoneal fluid in cases of acute pancreatitis and
blunt abdominal trauma by passing a spinal needle through the abdominal wall.
[31]
In 1965, Root et al
reported the use of percutaneous DPL in patients who had sustained blunt abdominal trauma.
[32]
DPL is used as a method of rapidly determining the presence of intraperitoneal blood. It is particularly useful
if the history and abdominal examination of an unstable patient with multisystem injuries are either unreliable
(eg, because of head injury, alcohol, or drug intoxication) or equivocal (eg, because of lower rib fractures,
pelvic fractures, or confounding clinical examination).
DPL is also useful for patients in whom serial abdominal examinations cannot be performed (eg, those in an
angiographic suite or operating room during emergency orthopedic or neurosurgical procedures).
[33]
DPL is indicated for the following patients in the setting of blunt trauma:
Patients with a spinal cord injury
Those with multiple injuries and unexplained shock
Obtunded patients with a possible abdominal injury
Intoxicated patients in whom abdominal injury is suggested
Patients with potential intra-abdominal injury who will undergo prolonged anesthesia for another
procedure
The only absolute contraindication to DPL is the obvious need for laparotomy. Relative contraindications
include morbid obesity, a history of multiple abdominal surgeries, and pregnancy.
Various methods of introducing the catheter into the peritoneal space have been described. These include
the open, semiopen, and closed methods. The open method requires an infraumbilical skin incision that is
extended to and through the linea alba. (In pregnant patients or in patients with particular risk for potential
pelvic hematoma, the incision should be placed superior to the umbilicus.) The peritoneum is opened, and
the catheter is inserted under direct visualization.
The semiopen method is identical, except that the peritoneum is not opened and the catheter is delivered
percutaneously through the peritoneum into the peritoneal cavity. The closed technique requires the catheter
to be inserted blindly through the skin, subcutaneous tissue, linea alba, and peritoneum.
The closed and semiopen techniques at the infraumbilical site are preferred at most centers. The fully open
method is the most technically demanding and is restricted to those situations in which the closed or
semiopen technique is unsuccessful or is deemed unsafe (eg, patients with pelvic fractures, pregnancy,
obesity, or prior abdominal operations).
After insertion of the catheter into the peritoneum, attempt to aspirate free intraperitoneal blood (at least 15-
20 mL). DPL results are considered positive in a blunt trauma patient if 10 mL of grossly bloody aspirate is
obtained before infusion of the lavage fluid or if the siphoned lavage fluid contains more than 100,000 red
blood cells (RBCs)/L, more than 500 white blood cells (WBCs)/L, elevated amylase content, bile, bacteria,
vegetable matter, or urine. Only approximately 30 mL of blood is needed in the peritoneum to produce a
microscopically positive DPL result.
If findings are negative, infuse 1 L of crystalloid solution (eg, lactated Ringer solution) into the peritoneum.
Then, allow this fluid to drain by gravity, and ensure that laboratory analysis is performed.
Complications of DPL include bleeding from the incision and catheter insertion, infection (ie, wound,
peritoneal), and injury to intra-abdominal structures (eg, urinary bladder, small bowel, uterus). These
complications may increase the possibility of false-positive studies. Additionally, infection of the incision,
peritonitis from the catheter placement, laceration of the urinary bladder, or injury to other intra-abdominal
organs can occur.
Bleeding from the incision, dissection, or catheter insertion can cause false-positive results that may lead to
unnecessary laparotomy. Achieve appropriate hemostasis prior to entering the peritoneum and placing the
catheter. False-positive DPL results can occur if an infraumbilical approach is used in a patient with a pelvic
fracture. A pelvic x-ray film should be obtained prior to performing DPL if a pelvic fracture is suggested.
Before DPL is attempted, the urinary bladder and stomach should be decompressed.
DPL has been shown in some studies to have a diagnostic accuracy of 98-100%, a sensitivity of 98-100%,
and a specificity of 90-96%. It has some advantages, including high sensitivity, rapidity, and immediate
interpretation. The main limitations of DPL include its potential for iatrogenic abdominal injury and its high
sensitivity, which can lead to nontherapeutic laparotomies.
With the availability of fast, noninvasive, and better imaging modalities (eg, FAST, CT scanning), the role of
DPL is now limited to the evaluation of unstable trauma patients in whom FAST results are negative or
inconclusive. In some contexts, DPL may be complemented with a CT scan if the patient has positive lavage
results but stabilizes.
Blunt Abdominal Trauma Treatment & Management
Prehospital Care
Prehospital care focuses on rapidly evaluating life-threatening problems, initiating resuscitative measures, and
initiating prompt transport to a definitive care site.
[34, 35]
The injured patient is at risk for progressive deterioration
from continued bleeding and requires rapid transport to a trauma center or the closest appropriate facility, with
appropriate stabilization procedures performed en route. Hence, securing the airway, placing large-bore
intravenous (IV) lines, and administering IV fluid must take place en route, unless transport is delayed.
A study by Nirula et al demonstrates the importance of field triage protocols that allow immediate transport to
definitive care sites for very severely injured patients.
[36]
In the study, the odds of death were 3.8 times greater for
patients initially triaged to a nontrauma center. Such responses require preplanning within a mature trauma system
and mandate appropriate prehospital training and protocols.
Use endotracheal intubation to secure the airway of any patient who is unable to maintain the airway or who has
potential airway threats. Secure the airway in conjunction with in-line cervical immobilization in any patient who
may have suffered cervical trauma. Provide artificial ventilation by using a high fraction of inspired oxygen (FIO2)
for patients who exhibit compromised breathing respirations. Maintain oxygen saturation (SaO2) at more than 90-
92%.
External hemorrhage rarely is associated with blunt abdominal trauma. If external bleeding is present, control it
with direct pressure. Note any signs of inadequate systemic perfusion. Consider intraperitoneal hemorrhage
whenever evidence of hemorrhagic shock is found in the absence of external hemorrhage.
Initiate volume resuscitation with crystalloid solution; however, never delay patient transport while IV lines are
inserted. En route, administer a fluid bolus of lactated Ringer or normal saline solution to patients with evidence of
shock.
[37, 38]
Titrate IV fluid therapy to the patients clinical response. Because overaggressive volume resuscitation may lead to
recurrent or increased hemorrhage, IV fluids should be titrated to a systolic blood pressure of 90-100 mm Hg. This
practice should provide the mean blood pressure necessary to maintain perfusion of the vital organs.
Acquire expeditious and complete spinal immobilization on patients with multisystem injuries and on patients with
a mechanism of injury that has potential for spinal cord trauma. In the rural setting, the pneumatic antishock
garment may have a role for treating shock resulting from a severe pelvic fracture.
Promptly notify the destination hospital so that that facility can activate its trauma team and prepare for the patient.
Emergency Department Care
Upon the patients arrival in the emergency department (ED) or trauma center, a rapid primary survey should be
performed to identify immediate life-threatening problems.
The first priority is reassessment of the airway. Protection of the cervical spine with in-line immobilization is
absolutely mandatory. If intubation is indicated, attempt nasotracheal (ie, if no contraindications) or endotracheal
intubation. If possible, perform and record a brief neurologic examination prior to neuromuscular blockade and
intubation. If intubation is unsuccessful, perform cricothyroidotomy (see the video below).
Surgical cricothyroidotomy Seldinger. Video courtesy of Therese Canares, MD, and Jonathan Valente, MD, Rhode Island
Hospital, Brown University.
After an airway has been established, adequate ventilatory exchange is assessed by auscultation of both lung
fields. Patients who display apnea or hypoventilation require respiratory support, as do those patients with
tachypnea. Provide all patients with supplemental oxygen from a device capable of delivering a high fraction of
inspired oxygen (FIO2) (eg, a nonrebreather mask).
Clinical diagnosis of a tension pneumothorax is treated with needle decompression followed by chest
thoracostomy tube placement. Other mechanical factors that can interfere with ventilation include sucking chest
wounds, a hemothorax, and pulmonary contusion. Treat these aggressively and expediently.
The next priority in the primary survey is an assessment of the circulatory status of the patient. Circulatory collapse
in a patient with blunt abdominal trauma is usually caused by hypovolemia from hemorrhage. Identification of
hypovolemia and signs of shock necessitate vigorous resuscitation and attempts to identify the source of blood
loss.
Effective volume resuscitation is accomplished by controlling external hemorrhage and infusing warmed crystalloid
solution via 2 large-bore (eg, 18-gauge) peripheral IV lines. Use central lines (preferably femoral by using a large-
bore line such as a Cordis catheter) and cutdowns (eg, saphenous, brachial) for patients in whom percutaneous
peripheral access cannot be established. Administer a rapid bolus of crystalloid.
Hemodynamic instability despite the administration of 2 L of fluid to adult patients indicates ongoing blood loss and
is an indication for immediate blood transfusion. Administer type O, Rh-negative blood if cross-matched or type-
specific blood is not available.
The CONTROL trial, the only prospective randomized trial of factor VII in trauma patients, evaluated the efficacy
and safety of recombinant factor VIIa as an adjunct to direct hemostasis in major trauma. Results showed a small
decrease in blood utilization but no mortality benefit. Currently available data do not support empiric use of factor
VIIa for civilian trauma patients.
[39]
The primary survey is completed with a brief neurologic assessment of the patient using elements of the Glasgow
Coma Scale (see the Glasgow Coma Scalecalculator). The patient is undressed and draped in clean, dry, warm
sheets.
After the primary survey and initial resuscitation have begun, complete the secondary survey, as described earlier
(see Physical Examination). Perform a thorough head-to-toe examination, paying attention to evidence of the
mechanism of injury and potentially injured areas. Before the placement of a nasogastric tube and Foley catheter,
perform appropriate head, neck, pelvic, perineum, and rectal examinations. Log-roll the patient to examine the
back and palpate the entire spinal column.
On the basis of the injury mechanism and the findings from physical examination, obtain initial trauma radiographic
studies. In general, trauma suite views include lateral cervical spine, anterior portable chest, and pelvis
radiographs. In-line spinal immobilization must be continued until spinal fractures have been ruled out. Additional
radiographs are indicated for other findings in the secondary survey.
Bedside ultrasonography using a trauma examination protocol (eg, FAST) can be used to determine the presence
of intraperitoneal hemorrhage (see the images below). If findings are negative or equivocal, DPL may be
performed in hemodynamically unstable patients.
Ultrasound image of right flank. Clear hypoechoic stripe exists between right kidney and liver in Morison pouch.
Ultrasound image of left flank in same patient, with thin hypoechoic stripe above spleen and wider hypoechoic stripe in
splenorenal recess.
Depending on patient stability, injury mechanism, and likelihood of intra-abdominal injury, further investigation may
be warranted for patients who are hemodynamically stable after the initial assessment and resuscitation and who
have negative or equivocal FAST or DPL results. Further investigation includes contrast-enhanced CT scans of
the abdomen and pelvis or serial examinations and ultrasonography.
Approach Considerations
Treatment of blunt abdominal trauma begins at the scene of the injury and is continued upon the patients arrival at
the emergency department (ED) or trauma center. Management may involve nonoperative measures or surgical
treatment, as appropriate.
Indications for laparotomy in a patient with blunt abdominal injury include the following:
Signs of peritonitis
Uncontrolled shock or hemorrhage
Clinical deterioration during observation
Hemoperitoneum findings after focused assessment with sonography for trauma (FAST) or diagnostic
peritoneal lavage (DPL) examinations
Finally, surgical intervention is indicated in patients with evidence of peritonitis based on physical examination
findings.
Operative treatment is not indicated in every patient with positive FAST scan results. Hemodynamically stable
patients with positive FAST findings may require a computed tomography (CT) scan to better define the nature
and extent of their injuries. Operating on every patient with positive FAST scan findings may result in an
unacceptably high laparotomy rate.
Resuscitative thoracotomy is not recommended in patients with blunt thoracoabdominal trauma who have
pulseless electrical activity upon arrival in the emergency department (ED). The survival rate in this situation is
virtually 0%. These patients may be allowed a thoracotomy in the ED only if they have signs of life upon arrival.
Nonoperative Management
Nonoperative management (NOM) strategies based on CT scan diagnosis and the hemodynamic stability of the
patient are now being used in adults for the treatment of solid organ injuries, primarily those to the liver and
spleen. In blunt abdominal trauma, including severe solid organ injuries, selective nonoperative management has
become the standard of care.
Angiography is a valuable modality in nonoperative management of abdominal solid organ injuries from blunt
trauma in adults. It is used aggressively for nonoperative control of hemorrhage, thereby obviating nontherapeutic
cost-inefficient laparotomies.
Splenic artery embolotherapy (SAE), although not standard of care, is another nonoperative management modality
for adult blunt splenic injury. Requarth et al conducted a metaanalysis comparing outcomes data for observational
management versus SAE by splenic injury grade cohort. Results show the failure rate of observational
management increases with splenic injury grade, whereas the failure rate of SAE does not change significantly
from splenic injury grades 1 to 5. In grade 4 and 5 injuries, SAE is associated with significantly higher salvage
rates. The SAE success rate noted may in part be due to the fact that SAE was introduced later in the experience
surveyed, and the improved NOM failure rate may be due to other factors that came into play as the experience
proceeded.
[40]
The trend toward simply observing hemodynamically stable patients with injuries involving the spleen, liver, or
kidneys is becoming more popular. In a study of pediatric patients, those with blunt abdominal trauma who were
hemodynamically stable after fluid replacement of less than 40 mL/kg, had proven evidence of solid organ injuries,
and remained stable were admitted to the pediatric intensive care unit (ICU) under surgical management. No
deaths and no immediate or long-term complications were reported in this group.
If the decision has been made to observe the patient, closely monitor vital signs and frequently repeat the physical
examination. An increased temperature or respiratory rate can indicate a perforated viscus or the formation of an
abscess. Pulse and blood pressure can also change with sepsis or intra-abdominal bleeding. Physical examination
findings reflecting peritonitis are an indication for surgical intervention.
Surgical Management
Resuscitative thoracotomy
Resuscitative thoracotomy in the ED is only occasionally life-saving. It is an aggressive, desperate measure
intended to save a patient whose death is thought to be imminent or otherwise inevitable. Survival with good
neurologic recovery is more likely for patients with penetrating trauma than for patients with blunt trauma.
Thoracotomy may have a role in selected patients with penetrating injuries to the neck, chest, or extremities and
those with signs of life within 5 minutes of arrival in the ED.
A resuscitative thoracotomy is seldom of benefit for patients with cardiac arrest secondary to blunt or head
injury or for those without vital signs at the scene of the accident. Patients with blunt thoracoabdominal trauma with
pulseless electrical activity upon arrival in the ED have a survival rate of virtually 0% and are poor candidates for
resuscitative thoracotomy. Patients with blunt trauma may be allowed a thoracotomy in the ED only if they have
signs of life upon arrival.
In a patient with hemoperitoneum from blunt thoracoabdominal trauma, the goals of a resuscitative thoracotomy in
the ED are (1) to cross-clamp the aorta, diverting available blood to the coronaries and cerebral vessels during
resuscitation; (2) to evacuate pericardial tamponade; (3) to directly control thoracic hemorrhage; and (4) to open
the chest for cardiac massage.
Laparotomy and definitive repair
Indications for laparotomy in a patient with blunt abdominal injury include signs of peritonitis, uncontrolled shock or
hemorrhage, clinical deterioration during observation, and hemoperitoneum findings after FAST or DPL
examinations (see Workup).
When laparotomy is indicated, broad-spectrum antibiotics are given. A midline incision is usually preferred. When
the abdomen is opened, hemorrhage control is accomplished by removing blood and clots, packing all 4
quadrants, and clamping vascular structures. Obvious hollow viscus injuries (HVIs) are sutured. After intra-
abdominal injuries have been repaired and hemorrhage has been controlled by packing, a thorough exploration of
the abdomen is then performed to evaluate the entire contents of the abdomen.
After intraperitoneal injuries are controlled, the retroperitoneum and pelvis must be inspected. Do not explore
pelvic hematomas. Use external fixation of pelvic fractures to reduce or stop blood loss in this region. Explore
large or expanding midline retroperitoneal hematomas, with the anticipation of damage to the large vascular
structures, pancreas, or duodenum. Do not explore small or stable perinephric hematomas.
After the source of bleeding has been stopped, further stabilizing the patient with fluid resuscitation and
appropriate warming is important. After such measures are complete, perform a thorough exploratory laparotomy
with appropriate repair of all injured structures.
A study by Crookes et al suggests that the true morbidity of a negative laparotomy may not be as high as
previously believed.
[41]
They conclude that in blunt abdominal trauma patients, exploratory laparotomy to establish a
diagnosis does not result in increased morbidity in a 30-day period, compared with no laparotomy. In other words,
it is safer to undergo laparotomy with negative findings than to delay treatment of an injury.
It must be stressed, however, that in this digital era with high-resolution imaging the need to take a patient for
exploratory laparotomy only to establish a diagnosis may be unnecessary and expensive if, for instance, the CT is
negative and the patient is hemodynamically stable.
Patients who had gross enteric contamination of the peritoneal cavity are given appropriate antibiotics for 5-7
days.
If a pelvic hematoma was found and the patient continues to lose blood after external fixation of a pelvic fracture,
arteriography with embolization can be used to stop the small percentage of arterial bleeding found in pelvic
fractures.
In adults, splenic artery embolization has been shown to improve nonoperative splenic salvage rates. A
retrospective review showed that this procedure may be useful in the adolescent population as well, particularly in
patients with high-grade injuries or with evidence of splenic vascular injury, although this is not the standard of
care.
[42]
Consultations
The best outcomes from trauma are obtained by involving consultants who possess specific expertise and training
in managing trauma patients. Consider evaluation by a trauma surgeon for all patients with evidence of blunt
abdominal trauma. Clearly, hemodynamic instability or the identification of significant abnormalities during physical
examination or a diagnostic procedure necessitates the involvement of a trauma surgeon.
Specific physical examination findings that call for timely surgical evaluation are as follows:
History of blunt abdominal trauma, shock, or abnormal vital signs (eg, tachycardia, hypotension)
Evidence of shock without obvious external blood loss
Evidence of peritonitis (eg, marked tenderness, involuntary guarding, percussion tenderness)
Findings consistent with potential intra-abdominal injury (eg, lap belt signs, lower rib fractures, lumbar spine
fractures)
Altered levels of consciousness or sensation, whether due to drugs, alcohol, or head/spinal injury
Patients who require other prolonged operative intervention (eg, orthopedic procedures)
Specific findings on diagnostic studies that call for timely surgical evaluation include evidence of free fluid or solid
organ injury on sonograms or CT scans.
Although a trend toward nonoperative management of hepatic, splenic, and renal injuries in patients who are
hemodynamically normal has occurred, a trained trauma surgeon must oversee this care.
Other specific findings that indicate timely trauma surgeon involvement are as follows:
Positive findings on DPL
Evidence of extravasated contrast or extraluminal air on an upper gastrointestinal series (eg, duodenal
rupture), plain abdominal radiography, or cystography
Serious pelvic fractures
Evidence of bladder rupture on contrast cystogram or gross hematuria
Elevated findings on liver function studies
If consultants with expertise in managing blunt abdominal injuries are unavailable, arrange patient transfer to the
nearest appropriate trauma center as soon as injury is identified. Lengthy diagnostic workup is counterproductive
once it is recognized that a patient cannot be managed at the initial facility. Physician-to-physician consultation
must occur before transport to ensure that the receiving facility has the resources necessary to care for the patient.
Long-Term Monitoring
Before discharge, provide patients with detailed instructions that describe signs of undiagnosed injury. Increased
abdominal pain or distention, nausea or vomiting, weakness, lightheadedness or fainting, or new bleeding in urine
or feces mandates immediate return and further evaluation. Ensure that close follow-up care and repeat
examinations are available for all patients.
Blunt Abdominal Trauma Medication
Medication Summary
Judiciously prescribe pain medications to patients who are discharged. To prevent masked or delayed
presentations, ensure that a close follow-up for reevaluation is available to all patients who are provided pain
medications. With the potential for hemorrhage, nonsteroidal anti-inflammatory drugs (NSAIDs) probably should be
avoided. Acetaminophen with or without small quantities of mild narcotic analgesics may be all that should be
prescribed initially. Minimize use of analgesics in patients who are admitted for observation.
Patients who undergo laparotomy may require routine perioperative antibiotics. Patients with repaired hollow organ
injury may require additional antibiotics.
Analgesics
Class Summary
Pain control is essential to quality patient care. It ensures patient comfort, promotes pulmonary toilet, and prevents
exacerbations in tachycardia and hypertension.
View full drug information
Morphine sulfate (Duramorph, Astramorph, MS Contin, Avinza, Kadian)
Morphine is the drug of choice for narcotic analgesia due to its reliable and predictable effects, safety profile, and
ease of reversibility with naloxone. Like fentanyl, morphine sulfate is easily titrated to desired level of pain control.
Morphine sulfate administered intravenously may be dosed in a number of ways. It is commonly titrated until the
desired effect is obtained.
View full drug information
Fentanyl citrate (Fentora, Abastral, Duragesic)
A synthetic opioid analgesic that is primarily a mu receptor agonist, fentanyl is 50-100 times more potent than
morphine. It has a short duration of action (1-2 h) and minimal cardiovascular effects, such as hypotension.
Respiratory depression is uncommon, but this effect lasts longer than its analgesic effect. Fentanyl is frequently
used in patient-controlled analgesia for relief of pain. Unlike morphine, fentanyl is not commonly associated with
histamine release.
View full drug information
Acetaminophen and hydrocodone (Vicodin, Lortab, Norco)
This drug combination is indicated for relief of moderate to severe pain.
View full drug information
Hydromorphone (Dilaudid)
Hydromorphone is a potent semisynthetic opiate agonist similar in structure to morphine. It is approximately 7-8
times as potent as morphine on mg-to-mg basis, with a shorter or similar duration of action.
Acetaminophen with codeine (Tylenol-3)
This combination is a mild narcotic analgesic. Provide the family with a small supply for use when pain severity is
greater than can be managed with acetaminophen alone. Counsel parents to use for severe pain only, not as the
first medication for each symptom.
Antibiotics
Class Summary
Empiric antimicrobial therapy must be comprehensive and should cover all likely pathogens in the context of the
clinical setting.
View full drug information
Cefazolin
Cefazolin is a first-generation semisynthetic cephalosporin, which, by binding to 1 or more penicillin-binding
proteins, arrests bacterial cell wall synthesis and inhibits bacterial replication. It has a poor capacity to cross the
blood-brain barrier. Cefazolin is primarily active against skin flora, including S aureus. Regimens for intravenous
and intramuscular dosing are similar. It is typically used alone for skin and skin-structure coverage.
View full drug information
Cephalexin (Keflex)
This is a first-generation cephalosporin that inhibits bacterial replication by inhibiting bacterial cell wall synthesis. It
is bactericidal and is effective against rapidly growing organisms forming cell walls.
Resistance occurs by the alteration of penicillin-binding proteins. Cephalexin is effective for treatment of infections
caused by streptococcal or staphylococcal organisms, including penicillinase-producing staphylococci. It may use
to initiate therapy when streptococcal or staphylococcal infection is suspected.
It is used orally when outpatient management is indicated.
Cefotaxime (Claforan)
Cefotaxime is a third-generation cephalosporin with a broad gram-negative spectrum, lower efficacy against gram-
positive organisms, and higher efficacy against resistant organisms. It acts by arresting bacterial cell wall synthesis
by binding to one or more penicillin-binding proteins, which, in turn, inhibits bacterial growth. Cefotaxime is used
for septicemia and treatment of gynecologic infections caused by susceptible organisms, but it has a lower efficacy
against gram-positive organisms.
View full drug information
Ceftazidime (Fortaz, Tazicef)
Ceftazidime is a third-generation cephalosporin with broad-spectrum, gram-negative activity, including
against Pseudomonas; it has low efficacy against gram-positive organisms and high efficacy against resistant
organisms. This agent arrests bacterial growth by binding to one or more penicillin-binding proteins, which, in turn,
inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell wall synthesis, thus inhibiting cell
wall biosynthesis.
The condition of the patient, severity of infection, and susceptibility of the microorganism should determine the
proper dose and route of administration.
View full drug information
Ceftriaxone (Rocephin)
Ceftriaxone is a third-generation cephalosporin with broad-spectrum gram-negative activity, low efficacy against
gram-positive organisms, and high efficacy against resistant organisms. It is considered the drug of choice for
parenteral agents in community-acquired pneumonia. Bactericidal activity results from the inhibition of cell wall
synthesis by binding to one or more penicillin-binding proteins. This agent exerts its antimicrobial effect by
interfering with the synthesis of peptidoglycan, a major structural component of the bacterial cell wall. Bacteria
eventually lyse due to ongoing activity of cell wall autolytic enzymes, while the cell wall assembly is arrested.
Ceftriaxone is highly stable in the presence of beta-lactamases, both penicillinase and cephalosporinase, and of
gram-negative and gram-positive bacteria. Approximately 33-67% of the dose is excreted unchanged in urine, and
the remainder is secreted in bile and, ultimately, in feces as microbiologically inactive compounds. This agent
reversibly binds to human plasma proteins, and binding has been reported to decrease from 95% bound at plasma
concentrations of less than 25 mcg/mL to 85% bound at 300 mcg/mL.
View full drug information
Erythromycin (E.E.S., Ery-Tab, Erythrocin, PCE, EryPed)
Erythromycin covers most potential etiologic agents, including Mycoplasmaspecies. The oral regimen may be
insufficient to adequately treat Legionellaspecies, and this agent is less active against H influenzae. Although the
standard course of treatment is 10 days, treatment until the patient has been afebrile for 3-5 days seems a more
rational approach. Erythromycin therapy may result in GI upset, causing some clinicians to prescribe an alternative
macrolide or change to a thrice-daily dosing.
Erythromycin is a macrolide that inhibits bacterial growth possibly by blocking dissociation of peptidyl t-RNA from
ribosomes, causing RNA-dependent protein synthesis to arrest.
View full drug information
Amoxicillin and clavulanate (Augmentin, Augmentin XR, Amoclan)
Amoxicillin inhibits bacterial cell wall synthesis by binding to penicillin-binding proteins. The addition of clavulanate
inhibits beta-lactamase producing bacteria.
It is a good alternative antibiotic for patients allergic to or intolerant of the macrolide class. It is usually is well
tolerated and provides good coverage to most infectious agents. It is not effective
against Mycoplasma and Legionella species. The half-life of the oral dosage form is 1-1.3 hours. It has good tissue
penetration but does not enter cerebrospinal fluid.
For children older than 3 months, base the dosing protocol on the amoxicillin content. Due to different
amoxicillin/clavulanic acid ratios in the 250-mg tablet (250/125) versus the 250-mg chewable tablet (250/62.5), do
not use the 250-mg tablet until child weighs more than 40 kg.
View full drug information
Ampicillin and sulbactam (Unasyn)
This is a drug combination of a beta-lactamase inhibitor with ampicillin. It interferes with bacterial cell wall
synthesis during active replication, causing bactericidal activity against susceptible organisms. It is an alternative
to amoxicillin when the patient is unable to take medication orally.
It covers skin, enteric flora, and anaerobes. It is not ideal for nosocomial pathogens.
View full drug information
Piperacillin and tazobactam sodium (Zosyn)
This is an antipseudomonal penicillin plus a beta-lactamase inhibitor. It inhibits the biosynthesis of cell wall
mucopeptide and is effective during the stage of active multiplication.
View full drug information
Ticarcillin and clavulanate (Timentin)
It inhibits the biosynthesis of cell wall mucopeptide and is effective during the stage of active growth.
It is an antipseudomonal penicillin plus a beta-lactamase inhibitor that provides coverage against most gram-
positives, most gram negatives, and most anaerobes.
View full drug information
Ciprofloxacin (Cipro)
Ciprofloxacin is a fluoroquinolone that inhibits bacterial DNA synthesis and, consequently, growth, by inhibiting
DNA gyrase and topoisomerases, which are required for replication, transcription, and translation of genetic
material. Quinolones have broad activity against gram-positive and gram-negative aerobic organisms. It is has no
activity against anaerobes. Continue treatment for at least 2 days (7-14 d typical) after signs and symptoms have
disappeared.
View full drug information
Levofloxacin (Levaquin)
Levofloxacin is rapidly becoming a popular choice in pneumonia; this agent is a fluoroquinolone used to treat
community-acquired pneumonia caused by S aureus, S pneumoniae (including penicillin-resistant strains), H
influenzae, H parainfluenzae, Klebsiella pneumoniae, M catarrhalis, C pneumoniae, Legionella pneumophila, or M
pneumoniae. Fluoroquinolones should be used empirically in patients likely to develop exacerbation due to
resistant organisms to other antibiotics.
Levofloxacin is the L stereoisomer of the D/L parent compound ofloxacin, the D form being inactive. It is good
monotherapy with extended coverage againstPseudomonas species and excellent activity against pneumococci.
Levofloxacin acts by inhibition of DNA gyrase activity. The oral form has a bioavailability that is reportedly 99%.
The 750-mg dose is as well tolerated as the 500-mg dose, and it is more effective. Other fluoroquinolones with
activity against S pneumoniae may be useful and include moxifloxacin, gatifloxacin, and gemifloxacin.
Clindamycin (Cleocin, Cleocin Pediatric)
Clindamycin is a lincosamide semisynthetic antibiotic produced by 7(S)-chloro-substitution of 7(R)-hydroxyl group
of the parent compound lincomycin. It inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA
from ribosomes, causing RNA-dependent protein synthesis to arrest. It widely distributes in the body, without
penetration of the CNS. It is protein bound and is excreted by the liver and kidneys.
It is available in a parenteral form (ie, clindamycin phosphate) and oral form (ie, clindamycin hydrochloride). Oral
clindamycin is absorbed rapidly and almost completely and is not appreciably altered by the presence of food in
the stomach. Appropriate serum levels are reached and sustained for at least 6 hours following an oral dose. No
significant levels are attained in cerebrospinal fluid. It is also effective against aerobic and anaerobic streptococci
(except enterococci).
http://emedicine.medscape.com/article/1980980-overview
You might also like
- Abdominal TraumaDocument8 pagesAbdominal Traumahatem alsrour100% (2)
- Pulmonary EmbolismDocument46 pagesPulmonary EmbolismThevashini Shridaran100% (1)
- Shock, HypovolemicDocument2 pagesShock, HypovolemicNadya Syafitri100% (2)
- Laparoscopic Appendectomy SurgeryDocument2 pagesLaparoscopic Appendectomy SurgeryNycoNo ratings yet
- Acute AppendicitisDocument11 pagesAcute AppendicitisMary Jual Pe CaytapNo ratings yet
- Hypertensive CrisesDocument42 pagesHypertensive Crisescabinetuldeigiena0% (2)
- Case Study Acute Lymphoid LeukemiaDocument1 pageCase Study Acute Lymphoid Leukemia2literNo ratings yet
- Abdominal Compartment SyndromeDocument9 pagesAbdominal Compartment SyndromeNina Kharima100% (1)
- Blunt Abdominal TraumaDocument23 pagesBlunt Abdominal TraumaKadek Adi WigunaNo ratings yet
- Hypovolemic Shock PathoDocument10 pagesHypovolemic Shock PathoLorebell100% (1)
- Modified Radical MastectomyDocument6 pagesModified Radical Mastectomymetch isulatNo ratings yet
- GERD PathophysiologyDocument35 pagesGERD PathophysiologyKathlea Noble-dc100% (1)
- Bladder TumorDocument32 pagesBladder TumorAngelynChristabellaNo ratings yet
- Acute PancreatitisDocument7 pagesAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- Intracerebral HemorrageDocument13 pagesIntracerebral HemorrageChristian JuarezNo ratings yet
- Benign Tumors of The StomachDocument55 pagesBenign Tumors of The Stomachapi-19641337No ratings yet
- Bladder CancerDocument1 pageBladder CancerCarmina AguilarNo ratings yet
- Case Presentation-Nasopharyngeal CarcinomaDocument18 pagesCase Presentation-Nasopharyngeal Carcinomatehkie04100% (3)
- Rectal CancerDocument4 pagesRectal CancerHaru Zenkonstein0% (1)
- Case Presentation Station 3B Drug Study TramadolDocument3 pagesCase Presentation Station 3B Drug Study TramadolhahahahaaaaaaaNo ratings yet
- Cardiac Tamponade REPOOOORTDocument37 pagesCardiac Tamponade REPOOOORTDep Silvestre100% (1)
- Buerger's DiseaseDocument5 pagesBuerger's Diseaseglie_e52164100% (5)
- Abdominal Compartment SyndromeDocument29 pagesAbdominal Compartment Syndromesgod34100% (1)
- Upper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaDocument40 pagesUpper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaAy Alex0% (1)
- PneumothoraxDocument52 pagesPneumothoraxtrisna satrianaNo ratings yet
- Abruptio PlacentaDocument8 pagesAbruptio PlacentaNutz TolentinoNo ratings yet
- Acute Liver Failure in Adults: Etiology, Clinical Manifestations, and Diagnosis - UpToDateDocument14 pagesAcute Liver Failure in Adults: Etiology, Clinical Manifestations, and Diagnosis - UpToDateIatros GarciniNo ratings yet
- Papillary CarcinomaDocument7 pagesPapillary Carcinomarazik89No ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathySuhas KandeNo ratings yet
- Case UreterolithiasisDocument26 pagesCase UreterolithiasisPutri Dwi Kartini0% (1)
- Septic ShockDocument48 pagesSeptic ShockAnggie Drei IcuNo ratings yet
- Intestinal Obstruction: Methas Arunnart MDDocument42 pagesIntestinal Obstruction: Methas Arunnart MDJhe-sie AngelinaNo ratings yet
- Dysfunctional Uterine BleedingDocument6 pagesDysfunctional Uterine Bleedingboorai^_^No ratings yet
- Bladder Cancer: By: Estigoy, Harriet and Galang, Cuttie AnneDocument18 pagesBladder Cancer: By: Estigoy, Harriet and Galang, Cuttie AnneCuttie Anne Galang100% (1)
- Nasopharyngeal Cancer CompleteDocument54 pagesNasopharyngeal Cancer CompleteAmemonsajaah AmemonNo ratings yet
- Colorectal CancerDocument50 pagesColorectal CancerHans Chester Rirao Capinding100% (2)
- Cardiac TamponadeDocument3 pagesCardiac TamponadeKimberly SolisNo ratings yet
- Rectal CarcinomaDocument16 pagesRectal Carcinomabuddy557No ratings yet
- Interactive Session On Sodium Homeostasis: Dr.M.Emmanuel Bhaskar Assistant Professor in Medicine SRMC & RiDocument64 pagesInteractive Session On Sodium Homeostasis: Dr.M.Emmanuel Bhaskar Assistant Professor in Medicine SRMC & Ridrbhaskar100% (4)
- Penetrating Abdominal TraumaDocument67 pagesPenetrating Abdominal TraumarizkaNo ratings yet
- Burns History TakingDocument8 pagesBurns History TakingHelena Meurial Hilkiah100% (1)
- Small Bowel ObstructionDocument2 pagesSmall Bowel ObstructionSrividya PushpalaNo ratings yet
- Cholecystolithiasis: Characteristics and CompositionDocument7 pagesCholecystolithiasis: Characteristics and Compositionjesabel_caraigNo ratings yet
- Esophageal VaricesDocument14 pagesEsophageal VaricesKarla So MejiaNo ratings yet
- Acute Myocardial InfarctionDocument20 pagesAcute Myocardial InfarctionDavid Christian CalmaNo ratings yet
- Upper Gastrointestinal Bleeding.Document13 pagesUpper Gastrointestinal Bleeding.Gieselle Scott100% (1)
- Pleural Effusion Case StudyDocument31 pagesPleural Effusion Case StudyHomework PingNo ratings yet
- Colorectal CancerDocument3 pagesColorectal CancerAriane May Rubio50% (2)
- Nursing Care Plan Renal FailureDocument11 pagesNursing Care Plan Renal Failurenosevad88850% (2)
- Triads in MedicineDocument4 pagesTriads in MedicineÐr SalmaNo ratings yet
- NCP DMDocument21 pagesNCP DMKate ManalastasNo ratings yet
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDocument20 pagesEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNo ratings yet
- Heart Failure COncept MapDocument2 pagesHeart Failure COncept MapJrBong SemaneroNo ratings yet
- TAHBSO ReportDocument4 pagesTAHBSO ReportsachiiMeNo ratings yet
- Intestinal ObstructionDocument27 pagesIntestinal ObstructionAna AvilaNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Guidelines For Air Medical Dispatch PDFDocument23 pagesGuidelines For Air Medical Dispatch PDFDen SinyoNo ratings yet
- Prehospital Triage and Emergency Room Care in TBIDocument6 pagesPrehospital Triage and Emergency Room Care in TBIDen SinyoNo ratings yet
- Disaster RecoveryDocument10 pagesDisaster RecoveryDen SinyoNo ratings yet
- Safe Intrahospital Transport of Critically III Ventilator-Dependent PatientsDocument3 pagesSafe Intrahospital Transport of Critically III Ventilator-Dependent PatientsDen SinyoNo ratings yet
- After The Disaster - Rebuilding Communities PDFDocument98 pagesAfter The Disaster - Rebuilding Communities PDFDen SinyoNo ratings yet
- Resuscitation MedicationDocument1 pageResuscitation MedicationDen SinyoNo ratings yet
- Alcohols OD TreatmentDocument7 pagesAlcohols OD TreatmentDen SinyoNo ratings yet
- Initial Assessment of Emergency Department PatientsDocument11 pagesInitial Assessment of Emergency Department PatientsDen Sinyo0% (1)
- Acute Respiratory Distress SyndromeDocument5 pagesAcute Respiratory Distress SyndromeDen SinyoNo ratings yet
- Epidemiology and Genetics of Sudden Cardiac DeathDocument18 pagesEpidemiology and Genetics of Sudden Cardiac DeathDen SinyoNo ratings yet
- Mini Telaah JurnalDocument9 pagesMini Telaah JurnalDen SinyoNo ratings yet
- Ghid DZ Ada EasdDocument16 pagesGhid DZ Ada Easdpanchoss2001No ratings yet
- ED Nurse OrientDocument2 pagesED Nurse OrientDen SinyoNo ratings yet
- Gambaran Uji Fungsi Paru Pada Anak Penderita AsmaDocument4 pagesGambaran Uji Fungsi Paru Pada Anak Penderita AsmaDen SinyoNo ratings yet
- Ce To Acidosis Diabetic ADocument23 pagesCe To Acidosis Diabetic AHuber MunozNo ratings yet
- Annales D 891 HÃ Tã Nen DissDocument85 pagesAnnales D 891 HÃ Tã Nen DissDen SinyoNo ratings yet
- Out 2Document14 pagesOut 2Den SinyoNo ratings yet
- Icd 11Document5 pagesIcd 11Ahtisham Alam GujjarNo ratings yet
- Jurnal ReadingDocument22 pagesJurnal Readingarismaputra20No ratings yet
- Ama Report of The Council On Science and Public Health Obesity As A DiseaseDocument14 pagesAma Report of The Council On Science and Public Health Obesity As A Diseaseapi-285790500No ratings yet
- Mental Health in IndiaDocument6 pagesMental Health in IndiaStarlin MythriNo ratings yet
- Farmacist Desk Reference ReviewDocument1 pageFarmacist Desk Reference ReviewThinh DoNo ratings yet
- Organizational Chart Tertiary LabDocument1 pageOrganizational Chart Tertiary LabMiki Nishihara86% (7)
- E047330 FullDocument10 pagesE047330 FullRachmi Saskia Husnika PutriNo ratings yet
- Pregnancy - Preparing To Be A MomDocument16 pagesPregnancy - Preparing To Be A MomTes B FourieNo ratings yet
- SOAP Notes-WPS OfficeDocument11 pagesSOAP Notes-WPS OfficeNexi anessaNo ratings yet
- Tubigon Bohol S Nutrition Programs and Best PracticesDocument27 pagesTubigon Bohol S Nutrition Programs and Best PracticesReuben Jr UmallaNo ratings yet
- Erythema Multiforme and HomoeopathyDocument7 pagesErythema Multiforme and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Activity 5 TitrationDocument1 pageActivity 5 TitrationPorcha PacsayNo ratings yet
- VTE Assessment & GuidelinesDocument2 pagesVTE Assessment & GuidelinesAgustreginaNo ratings yet
- Lec 5 New Castle DiseaseDocument38 pagesLec 5 New Castle Diseasebasit abdulNo ratings yet
- Dental Council - DR Ann Hahessy Undertaking - 20221007Document2 pagesDental Council - DR Ann Hahessy Undertaking - 20221007Saifullah KhanNo ratings yet
- Presentation How To Properly Fillout New CF2 For Z Ben v2Document25 pagesPresentation How To Properly Fillout New CF2 For Z Ben v2Richard SonsingNo ratings yet
- "Comparative Evaluation of Rate of Canine Retraction in Corticotomy Facilitated Orthodontics and Piezocision Technique in Adult Population" - Protocol For A in Vivo StudyDocument7 pages"Comparative Evaluation of Rate of Canine Retraction in Corticotomy Facilitated Orthodontics and Piezocision Technique in Adult Population" - Protocol For A in Vivo StudyAly OsmanNo ratings yet
- Acrylic Removable Partial Denture (RPD)Document6 pagesAcrylic Removable Partial Denture (RPD)israaNo ratings yet
- Cataract Symptoms Score Di Kota BandungDocument11 pagesCataract Symptoms Score Di Kota BandungSujidah Rajab100% (1)
- Behavior and Social SciencesDocument11 pagesBehavior and Social SciencesRoxana Alexandra BogosNo ratings yet
- MPH Curriculum ExampleDocument3 pagesMPH Curriculum ExampleMark EbrahimNo ratings yet
- PHC BONE & JOINT Conference BROCHURE 2012Document6 pagesPHC BONE & JOINT Conference BROCHURE 2012Shrikant KhangarNo ratings yet
- .. Uploads Lecture Implant Overdenture 200702Document21 pages.. Uploads Lecture Implant Overdenture 200702siddu76100% (1)
- Exercise & Diet: The Importance ofDocument2 pagesExercise & Diet: The Importance ofEve Jay TaboclaonNo ratings yet
- Teaching Slide Set 2021: Global Initiative For Chronic Obstructive Lung Disease (Gold)Document58 pagesTeaching Slide Set 2021: Global Initiative For Chronic Obstructive Lung Disease (Gold)hendra ritongaNo ratings yet
- 07 DomingopjvmfinalDocument9 pages07 DomingopjvmfinalyumixxiNo ratings yet
- PoultryDocument11 pagesPoultryTawanda MandazaNo ratings yet
- Prosto 1Document11 pagesProsto 1saliamaharaniNo ratings yet
- Lejour Reduction MammoplastyDocument6 pagesLejour Reduction MammoplastyMiguelito JohnsonNo ratings yet
- Methodical Instructions For Students For Practical Classes 2Document3 pagesMethodical Instructions For Students For Practical Classes 2Gorle bhargavNo ratings yet