You might also like
- Essential Oils Pocket Reference - Fifth EditionDocument206 pagesEssential Oils Pocket Reference - Fifth Editionbianca7893% (88)
- Voice and Speech DisordersDocument2 pagesVoice and Speech DisordersVishal Gaurav100% (1)
- Muscle Tension DysphoniaDocument2 pagesMuscle Tension DysphoniaJenny RandallNo ratings yet
- Essential Questions in Paediatrics For MRCPCH v2 PDFDocument208 pagesEssential Questions in Paediatrics For MRCPCH v2 PDFa4aboo100% (11)
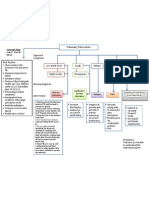
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Functional DysphoniaDocument5 pagesFunctional DysphoniaCati GallardoNo ratings yet
- Voice Treatment GuideDocument8 pagesVoice Treatment GuideburiramtourakomNo ratings yet
- Hyper NasalityDocument2 pagesHyper NasalityIsabelle MarquesNo ratings yet
- Efficacy of Water Resistance Therapy in Subjects Diagnosed With Behavioral Dysphonia: A Randomized Controlled TrialDocument10 pagesEfficacy of Water Resistance Therapy in Subjects Diagnosed With Behavioral Dysphonia: A Randomized Controlled TrialMatias GonzalezNo ratings yet
- Seminario Laryngeal Manual TherapyDocument14 pagesSeminario Laryngeal Manual TherapyDaniela Berndt PonceNo ratings yet
- Effects of Voice Therapy Using The Lip Trill Technique in P - 2019 - Journal ofDocument9 pagesEffects of Voice Therapy Using The Lip Trill Technique in P - 2019 - Journal ofJulia GavrashenkoNo ratings yet
- Differential Diagnosis DysarthriaDocument1 pageDifferential Diagnosis DysarthriaShruti KumarNo ratings yet
- Taxonomy Voice TherapyDocument26 pagesTaxonomy Voice TherapyCristina MeloNo ratings yet
- Lee SilvermanDocument13 pagesLee SilvermanLindsey BondNo ratings yet
- Voice and Voice Therapy BooneDocument37 pagesVoice and Voice Therapy BooneDEEKSHA ABROLNo ratings yet
- Communication ProblemDocument85 pagesCommunication ProblemHarshini SudharNo ratings yet
- Vocal Function Exercises For Presbylaryn PDFDocument9 pagesVocal Function Exercises For Presbylaryn PDFAngela Lleuful ToledoNo ratings yet
- Strech and Flow TherapyDocument9 pagesStrech and Flow TherapysopranopatriciaNo ratings yet
- The Value of Vocal Warm-Up and Cool-Down Exercises: Questions and ControversiesDocument3 pagesThe Value of Vocal Warm-Up and Cool-Down Exercises: Questions and ControversiesTayssa MarquesNo ratings yet
- Pediatric Voice PresentationDocument16 pagesPediatric Voice Presentationapi-254429093No ratings yet
- Voicecourse StrobosDocument35 pagesVoicecourse StrobospocepocNo ratings yet
- Voice Disorders 3Document9 pagesVoice Disorders 3Lalitha RajaNo ratings yet
- A Taxonomy of Voice TherapyDocument50 pagesA Taxonomy of Voice Therapydiana marcela mosquera acostaNo ratings yet
- Hoarseness of VoiceDocument6 pagesHoarseness of VoiceJayantiNo ratings yet
- EffectsofLaryngealCanceronVoice PDFDocument26 pagesEffectsofLaryngealCanceronVoice PDFSanNo ratings yet
- A Voice Rehabilitation Protocol With The SOVMDocument8 pagesA Voice Rehabilitation Protocol With The SOVMRachelNo ratings yet
- MedSLPCollective Handout Vocal Function ExercisesDocument8 pagesMedSLPCollective Handout Vocal Function ExercisesFenti FentikaNo ratings yet
- Voice Anatomy2Document49 pagesVoice Anatomy2Jerônimo Feitosa100% (1)
- PuberphoniaDocument15 pagesPuberphoniaZaini ZulqarnainNo ratings yet
- Puberphonia and Its ManagementDocument3 pagesPuberphonia and Its ManagementAnish RajNo ratings yet
- Efficacy of Stuttering Therapies - PDF /KUNNAMPALLIL GEJODocument24 pagesEfficacy of Stuttering Therapies - PDF /KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNo ratings yet
- SC10 Thomas LisaDocument113 pagesSC10 Thomas LisaAldo Hip Naranjo100% (1)
- Muscle Tension DysphoniaDocument3 pagesMuscle Tension DysphonianinaNo ratings yet
- MANAGEMENT FOR ADULTS WITH STUTTERING - PDF / KUNNAMPALLIL GEJODocument28 pagesMANAGEMENT FOR ADULTS WITH STUTTERING - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN100% (1)
- A Teacher's Voice - A Voical Hygiene Workshop-BL20Document23 pagesA Teacher's Voice - A Voical Hygiene Workshop-BL20AngelaNo ratings yet
- Enderby2013 Dysarthria Resumen PDFDocument9 pagesEnderby2013 Dysarthria Resumen PDFPatricio RomeroNo ratings yet
- Why Non Speech Oral Motor Exercises Are Not WarrantedDocument13 pagesWhy Non Speech Oral Motor Exercises Are Not WarrantedLoreto Opazo RojasNo ratings yet
- Titze 2015Document15 pagesTitze 2015Palito DuránNo ratings yet
- Classification Manual For Voice Disorders I PDFDocument297 pagesClassification Manual For Voice Disorders I PDFVerónicaCubillosNo ratings yet
- Quick Aphasia Battery (QAB) : 1. Level of ConsciousnessDocument39 pagesQuick Aphasia Battery (QAB) : 1. Level of ConsciousnessomeraNo ratings yet
- Speech Production: Music 318 Mini-Course On Speech and SingingDocument21 pagesSpeech Production: Music 318 Mini-Course On Speech and SingingSheila Marie RamosNo ratings yet
- Vocal AnatomyDocument8 pagesVocal AnatomyfunktotumNo ratings yet
- Paper Resonancia en Agua y Tubo EpilaringeoDocument8 pagesPaper Resonancia en Agua y Tubo EpilaringeoGonzalo NicolásNo ratings yet
- Theoretical Constructs in Fluency Development - PDF / KUNNAMPALLIL GEJODocument74 pagesTheoretical Constructs in Fluency Development - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN100% (1)
- Classification of Velopharyngeal DysfunctionDocument1 pageClassification of Velopharyngeal DysfunctionVictoria Rojas AlvearNo ratings yet
- A at Motor SpeechDocument5 pagesA at Motor SpeechNini JohannaNo ratings yet
- 2013 What Works - Speech Sound Disorders UpdateDocument26 pages2013 What Works - Speech Sound Disorders UpdatemariaNo ratings yet
- Phonation + Laryngeal Physiology: January 14, 2010Document46 pagesPhonation + Laryngeal Physiology: January 14, 2010Farhan HasbiNo ratings yet
- Biomechanics of Open Bite TreatmentDocument40 pagesBiomechanics of Open Bite TreatmentMaitreye PriyadarshiniNo ratings yet
- Laryngeal Massage Therapy-1Document7 pagesLaryngeal Massage Therapy-1filipamaltezNo ratings yet
- Hyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Effectiveness of Semi-Occluded Vocal Tract Exercises (Sovtes) in Patients With Dysphonia: A Systematic Review and Meta-AnalysisDocument19 pagesEffectiveness of Semi-Occluded Vocal Tract Exercises (Sovtes) in Patients With Dysphonia: A Systematic Review and Meta-AnalysisDANIELA IGNACIA FERNÁNDEZ LEÓNNo ratings yet
- Management For Multiple HandicapDocument57 pagesManagement For Multiple HandicapMSc Audio BNo ratings yet
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocument9 pagesAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiNo ratings yet
- Development of StutteringDocument8 pagesDevelopment of StutteringSiha SalamNo ratings yet
- MTPerspectives Jtamplin DysarthriaDocument9 pagesMTPerspectives Jtamplin DysarthriaAgustina IturriNo ratings yet
- Speech MechanismDocument34 pagesSpeech MechanismErl Dy0% (1)
- Voice Evaluation and Therapy: Key PointsDocument12 pagesVoice Evaluation and Therapy: Key PointsFátima MolinaNo ratings yet
- Videofluoroscopic Swallow Study - FinalDocument18 pagesVideofluoroscopic Swallow Study - Finalkir4_yamat0No ratings yet
- Voice Therapy TechniquesDocument15 pagesVoice Therapy TechniquesSingh Sikendrakumar100% (2)
- A Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Clinical Practice Guideline: Benign Paroxysmal Positional VertigoDocument35 pagesClinical Practice Guideline: Benign Paroxysmal Positional Vertigoapi-19500641No ratings yet
- Endoscopic DacryocystorhinostomyDocument17 pagesEndoscopic Dacryocystorhinostomyapi-19500641No ratings yet
- Superior Canal Dehiscence: Review of A New ConditionDocument7 pagesSuperior Canal Dehiscence: Review of A New Conditionapi-19500641No ratings yet
- Traditional Approaches To The OrbitDocument15 pagesTraditional Approaches To The Orbitapi-19500641No ratings yet
- Anatomy of The Orbit, Lacrimal and Lateral Nasal WallDocument10 pagesAnatomy of The Orbit, Lacrimal and Lateral Nasal Wallmadhurakavi shashiNo ratings yet
- The Pathophysiology of CholesteatomaDocument17 pagesThe Pathophysiology of Cholesteatomaapi-19500641No ratings yet
- Congenital Cholesteatoma TheoriesDocument14 pagesCongenital Cholesteatoma Theoriesapi-19500641No ratings yet
- Revision MastoidectomyDocument18 pagesRevision Mastoidectomyapi-19500641100% (1)
- Revision OssiculoplastyDocument14 pagesRevision Ossiculoplastyapi-19500641No ratings yet
- Revision StapedectomyDocument21 pagesRevision Stapedectomyapi-19500641100% (1)
- Laryngeal ElectromyographyDocument21 pagesLaryngeal Electromyographyapi-19500641No ratings yet
- Voice Therapy For The Professional VoiceDocument17 pagesVoice Therapy For The Professional Voiceapi-19500641100% (5)
- The Evolution of Surgical TrainingDocument9 pagesThe Evolution of Surgical Trainingapi-19500641No ratings yet
- Anesthesia, Antisepsis, MicroscopeDocument23 pagesAnesthesia, Antisepsis, Microscopeapi-19500641No ratings yet
- Intracranial Pressure Concerns in LateralDocument8 pagesIntracranial Pressure Concerns in Lateralapi-19500641No ratings yet
- Operative ProcedureDocument22 pagesOperative Procedurezianab aliNo ratings yet
- Immnunology Notebook Chapter One: Innate ImmunityDocument45 pagesImmnunology Notebook Chapter One: Innate ImmunityJavier Alejandro Daza GalvánNo ratings yet
- 2020 Anaphylaxis JACI 2020Document42 pages2020 Anaphylaxis JACI 2020Peter Albeiro Falla CortesNo ratings yet
- Knowledge, Attitude and Practices Towards Breast Feeding Among Lactating Mothers in King George Hospital, A Tertiary Care CenterDocument10 pagesKnowledge, Attitude and Practices Towards Breast Feeding Among Lactating Mothers in King George Hospital, A Tertiary Care CenterIJAR JOURNALNo ratings yet
- Is Doa 10 Cup TestDocument1 pageIs Doa 10 Cup TestUqi.No ratings yet
- Glaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionDocument9 pagesGlaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionFranco Paolo Maray-GhigliottoNo ratings yet
- On and Off Male Birth Control MethodsDocument2 pagesOn and Off Male Birth Control MethodsLeón L.PNo ratings yet
- Feeling GreatDocument243 pagesFeeling GreatSunny LamNo ratings yet
- BIO 211 Chapter 18 AssignmentDocument20 pagesBIO 211 Chapter 18 Assignmentf1l2o3r4e5n6No ratings yet
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocument5 pagesChronic Inflammatory Demyelinating PolyradiculoneuropathyDiego Fernando AlegriaNo ratings yet
- 1.0 Thrombocytes SCDocument10 pages1.0 Thrombocytes SC西矢椛No ratings yet
- PMLSDocument9 pagesPMLSChan ChanNo ratings yet
- HIV Drug Chart (2021)Document1 pageHIV Drug Chart (2021)savNo ratings yet
- Chest Pain FinalDocument17 pagesChest Pain FinalVarun R'MenonNo ratings yet
- Acadia PharmaceuticalsDocument3 pagesAcadia PharmaceuticalsAman DecoraterNo ratings yet
- Manual of Bone Densitometry Measurements - An Aid To The Interpretation of Bone Densitometry Measurements in A Clinical Setting PDFDocument229 pagesManual of Bone Densitometry Measurements - An Aid To The Interpretation of Bone Densitometry Measurements in A Clinical Setting PDFsesjrsNo ratings yet
- WellCat Veterinary HandbookDocument36 pagesWellCat Veterinary HandbookKatSiebrecht100% (5)
- Vitamin and Mineral Supplementation During PregnanDocument4 pagesVitamin and Mineral Supplementation During PregnanEvi RachmawatiNo ratings yet
- SVTDocument31 pagesSVTAkbar IskandarNo ratings yet
- Understanding The RelapseDocument12 pagesUnderstanding The RelapseruziyanaNo ratings yet
- Sports DrinksDocument2 pagesSports DrinksMustofaNo ratings yet
- Tercera SemanaDocument9 pagesTercera SemanaJesús Torres MayaNo ratings yet
- Physics and Imaging in Radiation OncologyDocument6 pagesPhysics and Imaging in Radiation Oncologydarr artNo ratings yet
- Mental IllnessDocument3 pagesMental IllnessKate EvangelistaNo ratings yet
- The Aao "At-A-Glance" Guide To CDT 2021 Orthodontic Codes: DentitionDocument2 pagesThe Aao "At-A-Glance" Guide To CDT 2021 Orthodontic Codes: DentitionSweet ToothNo ratings yet
- Carotid Sinus Massage - MuraliDocument31 pagesCarotid Sinus Massage - MuraliAhsan MohammedNo ratings yet
- XXXXXX 121Document11 pagesXXXXXX 121AndriantkNo ratings yet