You might also like
- Clinical Practice Guideline: Benign Paroxysmal Positional VertigoDocument35 pagesClinical Practice Guideline: Benign Paroxysmal Positional Vertigoapi-19500641No ratings yet
- Superior Canal Dehiscence: Review of A New ConditionDocument7 pagesSuperior Canal Dehiscence: Review of A New Conditionapi-19500641No ratings yet
- Mechanical EndonasalDocument18 pagesMechanical Endonasalapi-19500641No ratings yet
- Congenital Cholesteatoma TheoriesDocument14 pagesCongenital Cholesteatoma Theoriesapi-19500641No ratings yet
- Revision StapedectomyDocument21 pagesRevision Stapedectomyapi-19500641100% (1)
- Endoscopic ManagementDocument11 pagesEndoscopic Managementapi-19500641No ratings yet
- Endoscopic DacryocystorhinostomyDocument17 pagesEndoscopic Dacryocystorhinostomyapi-19500641No ratings yet
- Eustachian Tube FunctionDocument15 pagesEustachian Tube Functionapi-19500641No ratings yet
- Anatomy of The Orbit, Lacrimal and Lateral Nasal WallDocument10 pagesAnatomy of The Orbit, Lacrimal and Lateral Nasal Wallmadhurakavi shashiNo ratings yet
- Traditional Approaches To The OrbitDocument15 pagesTraditional Approaches To The Orbitapi-19500641No ratings yet
- Indications and TechniqueDocument19 pagesIndications and Techniqueapi-19500641100% (1)
- Complications of Chronic OtitisDocument19 pagesComplications of Chronic Otitisapi-19500641No ratings yet
- The Challenges of Revision SkullDocument17 pagesThe Challenges of Revision Skullapi-19500641No ratings yet
- Revision MastoidectomyDocument18 pagesRevision Mastoidectomyapi-19500641100% (1)
- The Pathophysiology of CholesteatomaDocument17 pagesThe Pathophysiology of Cholesteatomaapi-19500641No ratings yet
- Neurolaryngologic EvaluationDocument19 pagesNeurolaryngologic Evaluationapi-19500641No ratings yet
- Revision OssiculoplastyDocument14 pagesRevision Ossiculoplastyapi-19500641No ratings yet
- Revision Facial Nerve SurgeryDocument18 pagesRevision Facial Nerve Surgeryapi-19500641No ratings yet
- StrobovideolaryngosDocument11 pagesStrobovideolaryngosapi-19500641No ratings yet
- Cochlear ImplantsDocument10 pagesCochlear Implantsapi-19500641100% (1)
- Voice SurgeryDocument33 pagesVoice Surgeryapi-19500641No ratings yet
- Revision Cochlear ImplantationDocument7 pagesRevision Cochlear Implantationapi-19500641No ratings yet
- Vocal Fold Paresis and ParalysisDocument23 pagesVocal Fold Paresis and Paralysisapi-19500641No ratings yet
- Physical Examination of VoiceDocument17 pagesPhysical Examination of Voiceapi-19500641No ratings yet
- Vocal Fold MassesDocument18 pagesVocal Fold Massesapi-19500641No ratings yet
- Laryngeal ElectromyographyDocument21 pagesLaryngeal Electromyographyapi-19500641No ratings yet
- Vocal EmergenciesDocument18 pagesVocal Emergenciesapi-19500641No ratings yet
- Effects of Medications On The VoiceDocument10 pagesEffects of Medications On The Voiceapi-19500641No ratings yet
- Medical History in Voice ProfessionalsDocument21 pagesMedical History in Voice Professionalsapi-19500641No ratings yet
- Common Diagnoses and TreatmentsDocument37 pagesCommon Diagnoses and Treatmentsapi-19500641100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- WFNS Neuroanatomy Committee 3rd WebinarDocument4 pagesWFNS Neuroanatomy Committee 3rd WebinarhalikalifhayaNo ratings yet
- Surgical Ultrasound PT. Tawada Training August 18-21th, 2021Document46 pagesSurgical Ultrasound PT. Tawada Training August 18-21th, 2021Munawir gozaliNo ratings yet
- Schramm A., Gellrich N-C., Schmelzeisen R.-Navigational Surgery of The Facial Skeleton (2007)Document172 pagesSchramm A., Gellrich N-C., Schmelzeisen R.-Navigational Surgery of The Facial Skeleton (2007)Remus ChirciuNo ratings yet
- Attitudes and Perceptions of Omani Medical Students and Interns Toward Neurosurgery: A Cross-Sectional StudyDocument7 pagesAttitudes and Perceptions of Omani Medical Students and Interns Toward Neurosurgery: A Cross-Sectional Studymuhammad fahrizaNo ratings yet
- Global Neurosurgery The Current Capacity and DeficDocument11 pagesGlobal Neurosurgery The Current Capacity and DeficStefanus AlexanderNo ratings yet
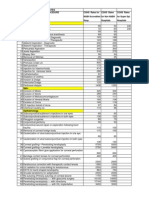
- Cghs Rates 2010Document25 pagesCghs Rates 2010Lincoln GnanadasNo ratings yet
- Vaibhav Super Specialty HospitalDocument101 pagesVaibhav Super Specialty Hospitalvaibhavkamdar100% (6)
- 2024 LHC 205Document31 pages2024 LHC 205WaqasSanaNo ratings yet
- Work Breakdown StructureDocument20 pagesWork Breakdown StructureUday100% (1)
- Endoscopic Surgery of The Orbit (Raj Sindwani)Document307 pagesEndoscopic Surgery of The Orbit (Raj Sindwani)sinclair Brice KINATA-BAMBINONo ratings yet
- A Patient With Massive Pneumocephalus Without Sign of Tension PneumocephalusDocument3 pagesA Patient With Massive Pneumocephalus Without Sign of Tension PneumocephalusImagen Gea GonzalezNo ratings yet
- Recognized Ho So ListDocument77 pagesRecognized Ho So Listdp663668No ratings yet
- The Economic Value of A Neurosurgeon To A HospitalDocument6 pagesThe Economic Value of A Neurosurgeon To A Hospitalmorris_tyoNo ratings yet
- National Hospital For Neurology and Neurosurgery Interactive Guide BrochureDocument49 pagesNational Hospital For Neurology and Neurosurgery Interactive Guide Brochuregorill4No ratings yet
- List of Empanelled HCOs-Pune (Dec 2020)Document15 pagesList of Empanelled HCOs-Pune (Dec 2020)GATE FACULTYNo ratings yet
- Guidelines For Management of Acute Cervical Spinal InjuriesDocument202 pagesGuidelines For Management of Acute Cervical Spinal InjuriesMuhammad IrfanNo ratings yet
- Home Microsurgical LabDocument11 pagesHome Microsurgical LabIevgenii IarmoliukNo ratings yet
- OxfordMedicineLIVETitleList NOV 2017 UpdatedDocument288 pagesOxfordMedicineLIVETitleList NOV 2017 UpdatedvladanNo ratings yet
- List of Empanelled HCOs - Delhi & NCR (24 June 2021)Document97 pagesList of Empanelled HCOs - Delhi & NCR (24 June 2021)rupeshNo ratings yet
- Minimally Invasive Spine Surgery NSDocument192 pagesMinimally Invasive Spine Surgery NSMihai CostacheNo ratings yet
- Brain Injury: Closed (Blunt) Brain Injury Occurs When The Head Accelerates and ThenDocument7 pagesBrain Injury: Closed (Blunt) Brain Injury Occurs When The Head Accelerates and Thencute_tineeNo ratings yet
- Prof - Dr.med - Habil Tarek A L - ZainDocument3 pagesProf - Dr.med - Habil Tarek A L - Zainprof.dr.tarek al-zain100% (2)
- CDH Sextant II ST Mdt18802Document48 pagesCDH Sextant II ST Mdt18802Choong Tze ShanNo ratings yet
- Ro-Jharkhand: List of Empanelled Hospitals Under Esic RegionDocument5 pagesRo-Jharkhand: List of Empanelled Hospitals Under Esic RegionShaina Hayat KhanNo ratings yet
- Do No Harm by Henry Marsh Chapter 1Document15 pagesDo No Harm by Henry Marsh Chapter 1The Sunday Times90% (10)
- 19-Microendoscopic Lumbar DiscectomyDocument8 pages19-Microendoscopic Lumbar DiscectomyNewton IssacNo ratings yet
- Cranioplasty After Traumatic Brain InjuryDocument5 pagesCranioplasty After Traumatic Brain InjuryGrnitrv 22No ratings yet
- Hospitals and Diagnostic CentreDocument32 pagesHospitals and Diagnostic CentreMurmu BricksNo ratings yet
- Medical Device Sales Representative in Buffalo NY Resume Stephen KleeDocument2 pagesMedical Device Sales Representative in Buffalo NY Resume Stephen KleeStephenKleeNo ratings yet
- Hard Device NeurosugeryDocument7 pagesHard Device NeurosugeryAditya Angga DharmaNo ratings yet