You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cellular Regulation - Nursing Test QuestionsDocument124 pagesCellular Regulation - Nursing Test QuestionsRNStudent1100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- CSC Competencies ModifiedDocument12 pagesCSC Competencies ModifiedCamille Junio100% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Panerai Catalogue 2012Document160 pagesPanerai Catalogue 2012M.Nazri Tan100% (1)
- Astm D6978-05 (2019)Document3 pagesAstm D6978-05 (2019)Chulaka PitigalaNo ratings yet
- Quality Update: Top Ten Questions For All Staff MembersDocument2 pagesQuality Update: Top Ten Questions For All Staff MembersCamille JunioNo ratings yet
- DD Preparations List - Updated 09.30. 2019Document15 pagesDD Preparations List - Updated 09.30. 2019Camille JunioNo ratings yet
- Record LabelsDocument60 pagesRecord LabelsCamille JunioNo ratings yet
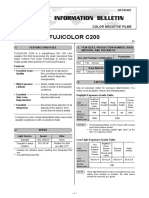
- Fujicolor C200: Color Negative FilmsDocument6 pagesFujicolor C200: Color Negative FilmsCamille JunioNo ratings yet
- Fujicolor C200: Color Negative FilmsDocument6 pagesFujicolor C200: Color Negative FilmsCamille JunioNo ratings yet
- Ovp Es2019Document5 pagesOvp Es2019Camille JunioNo ratings yet
- Credential: R.O.C. (Taiwan) National YesDocument4 pagesCredential: R.O.C. (Taiwan) National YesCamille JunioNo ratings yet
- Anu Foundation ConditionsDocument2 pagesAnu Foundation ConditionsCamille JunioNo ratings yet
- TourbillonDocument19 pagesTourbillonCamille JunioNo ratings yet
- General Guidelines (Artist)Document2 pagesGeneral Guidelines (Artist)Camille JunioNo ratings yet
- Rules of Inference and ReplacementDocument4 pagesRules of Inference and ReplacementCamille JunioNo ratings yet
- Pharmacy Calculations PDFDocument78 pagesPharmacy Calculations PDFGeorge John Amegashie100% (3)
- UP Diliman Dorm Rates 2011Document1 pageUP Diliman Dorm Rates 2011Camille JunioNo ratings yet
- Breaking Bond of MarriageDocument8 pagesBreaking Bond of MarriageCamille JunioNo ratings yet
- Criminal Procedure Act of TanzaniaDocument158 pagesCriminal Procedure Act of TanzaniaCamille JunioNo ratings yet
- PLJ Volume 11 Number 8 - 02 - Prof. Francisco Capistrano - The Revised Penal CodeDocument12 pagesPLJ Volume 11 Number 8 - 02 - Prof. Francisco Capistrano - The Revised Penal Codestephanie_patiño_4No ratings yet
- R.A. 8533 Family LawDocument1 pageR.A. 8533 Family LawCamille JunioNo ratings yet
- Fa10 Syllabus Ay13-14Document3 pagesFa10 Syllabus Ay13-14Camille JunioNo ratings yet
- Test InstructionDocument11 pagesTest InstructionlmlNo ratings yet
- Philippine CitizenshipDocument35 pagesPhilippine Citizenshipmountain_girlNo ratings yet
- Scenarios Where Child Product of Annulment Still LegitimateDocument11 pagesScenarios Where Child Product of Annulment Still LegitimateHappynako WholesomeNo ratings yet
- Odesk Contractor Manual 2013Document22 pagesOdesk Contractor Manual 2013shai1016No ratings yet
- Campus Map For Up DilimanDocument1 pageCampus Map For Up DilimanHanz FerrerNo ratings yet
- Unearthed Omega Calibre 560 RaritiesDocument10 pagesUnearthed Omega Calibre 560 RaritiesCamille JunioNo ratings yet
- Criminal Law Reviewer by Elmer BrabanteDocument267 pagesCriminal Law Reviewer by Elmer BrabanteCamille Junio100% (1)
- Application For Driver's License FormDocument2 pagesApplication For Driver's License FormOliver380100% (2)
- Graphic Design ComponentsDocument33 pagesGraphic Design ComponentsCamille JunioNo ratings yet
- Selenium 8Document14 pagesSelenium 8Tijesunimi AjayiNo ratings yet
- Baking Soda A Cure For HumanityDocument6 pagesBaking Soda A Cure For Humanitysheriff77080% (5)
- Bromelain A Potential Bioactive Compound: A Comprehensive Overview From A Pharmacological PerspectiveDocument26 pagesBromelain A Potential Bioactive Compound: A Comprehensive Overview From A Pharmacological PerspectiveMehdi BnsNo ratings yet
- Role of High Dose Methotrexate in Osteosarcoma - FinalDocument30 pagesRole of High Dose Methotrexate in Osteosarcoma - FinalHemanth KumarNo ratings yet
- ChemotherapyDocument11 pagesChemotherapyMaria Fudji HastutiNo ratings yet
- AGQ Cliff NotesDocument42 pagesAGQ Cliff NotesMitchellFelixNo ratings yet
- Multiple Choice Questions-Cancers: AdvertisementDocument5 pagesMultiple Choice Questions-Cancers: AdvertisementSp PpvNo ratings yet
- Learning Outcomes Chapter 16-Lewis Medical SurgicalDocument11 pagesLearning Outcomes Chapter 16-Lewis Medical Surgicalfirestartergirl100% (1)
- 2.7 Cell Division Going Wrong - Cancer-SNC2DDocument2 pages2.7 Cell Division Going Wrong - Cancer-SNC2DBob Dharam0% (1)
- Presentation Small Cell Lung CancerDocument59 pagesPresentation Small Cell Lung Cancerprudhviraj mNo ratings yet
- Guidelines Leptomeningeal MetastasisDocument16 pagesGuidelines Leptomeningeal MetastasisForem ZayneNo ratings yet
- The Most Powerful Anti-Cancer Agent: Vertes Papaya Leaf TeaDocument3 pagesThe Most Powerful Anti-Cancer Agent: Vertes Papaya Leaf TeajohnnyorithroNo ratings yet
- Chi1 PDFDocument17 pagesChi1 PDFchidambaramrNo ratings yet
- Development of Fludarabine FormulationsDocument12 pagesDevelopment of Fludarabine FormulationshamzaNo ratings yet
- Hematological Systems - Lecture NotesDocument15 pagesHematological Systems - Lecture NotesAmiel Francisco ReyesNo ratings yet
- 2 Week Diet AssignmentDocument40 pages2 Week Diet Assignmentapi-351011524No ratings yet
- Capecitabine IrinotecanDocument7 pagesCapecitabine Irinotecantanasa adrianNo ratings yet
- Chronic Lymphocytic LeukemiaDocument11 pagesChronic Lymphocytic LeukemiaCrisantaCasli100% (1)
- Osteosarcoma 1Document9 pagesOsteosarcoma 1Md Ahsanuzzaman PinkuNo ratings yet
- Aflori, Magdalena - Intelligent Polymers For Nanomedicine and biotechnologies-CRC Press (2018) PDFDocument243 pagesAflori, Magdalena - Intelligent Polymers For Nanomedicine and biotechnologies-CRC Press (2018) PDFcarquerNo ratings yet
- Cyclophosphamide Monograph 1june2013 FormattedDocument12 pagesCyclophosphamide Monograph 1june2013 Formattedpricilia ardianiNo ratings yet
- Dolly Madan Synopsis Lay OutDocument7 pagesDolly Madan Synopsis Lay OutBheeshm SinghNo ratings yet
- Brain TumorsDocument34 pagesBrain TumorsbenedictusNo ratings yet
- Afectiuni Lipire PlasturiDocument19 pagesAfectiuni Lipire PlasturilumidelinoNo ratings yet
- Surgical Management of Oral Pathological LesionDocument24 pagesSurgical Management of Oral Pathological Lesionمحمد ابوالمجدNo ratings yet
- Magic TrailDocument10 pagesMagic Trailchootu509No ratings yet
- Anti-Cancer SUDocument25 pagesAnti-Cancer SUAmmad FazilNo ratings yet
- Docking AnticancerDocument9 pagesDocking Anticanceradeliyaa khansaNo ratings yet