You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Tai Chi Code - Martial Arts Ebook by Chris DavisDocument190 pagesThe Tai Chi Code - Martial Arts Ebook by Chris DavisTomas De Wael100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Blood Doping PPT PresentationDocument26 pagesBlood Doping PPT Presentationee4254100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Staar Eoc 2016test Bio F 7Document39 pagesStaar Eoc 2016test Bio F 7api-293216402No ratings yet
- Manage Your Personal Energy PDFDocument46 pagesManage Your Personal Energy PDFezhil manickamNo ratings yet
- Approved LaboratoriesDocument22 pagesApproved LaboratoriesPaul CNo ratings yet
- Study Guide Cardio Tayang by Gextha 30 Maret 2015Document82 pagesStudy Guide Cardio Tayang by Gextha 30 Maret 2015Adi ParamarthaNo ratings yet
- Alvin MDocument2 pagesAlvin MRunmel Emmanuel Ramal DampiosNo ratings yet
- Tomasello, M. (2000) - Culture and Cognitive Development.Document4 pagesTomasello, M. (2000) - Culture and Cognitive Development.Roberto OcampoNo ratings yet
- Meriem Chatti - RéférencesDocument22 pagesMeriem Chatti - RéférencesOussama SghaïerNo ratings yet
- Capsicum Annuum L., Commonly Known As Hot Pepper or Chilli Is ADocument11 pagesCapsicum Annuum L., Commonly Known As Hot Pepper or Chilli Is Ajavedsaqi100% (1)
- 300 One Word Substitutions Asked in SSC IBPS UPSC ExamDocument12 pages300 One Word Substitutions Asked in SSC IBPS UPSC ExamRashid AliNo ratings yet
- Anatomy ReviewerDocument5 pagesAnatomy ReviewerPHILYP EPHRAIM PARANGALANNo ratings yet
- Hierarchy ExampleDocument18 pagesHierarchy ExampleSanket SahuNo ratings yet
- Using STADEN For Sequence AssemblyDocument5 pagesUsing STADEN For Sequence AssemblyChristen Rune StensvoldNo ratings yet
- The Effect of Temperature On The Reaction Time of The Enzyme Peroxidase - Lab ReportDocument5 pagesThe Effect of Temperature On The Reaction Time of The Enzyme Peroxidase - Lab ReportAnonymous aZEERFhvNo ratings yet
- Proposed Pre Final-1 Time Table With Weightage.. MPC, Bipc&Civils-AP&TsDocument17 pagesProposed Pre Final-1 Time Table With Weightage.. MPC, Bipc&Civils-AP&TsAbhiram muddanaNo ratings yet
- MHE RDG Wonders LVRDR G3 ELL U4W3 18Document24 pagesMHE RDG Wonders LVRDR G3 ELL U4W3 18Kenneth N AngelineNo ratings yet
- Taxonomy of Haematococcus PluvialisDocument2 pagesTaxonomy of Haematococcus PluvialisKomathi BalasupramaniamNo ratings yet
- ALB2Document4 pagesALB2Jonalyn SalandoNo ratings yet
- Tule Elk in Point ReyesDocument4 pagesTule Elk in Point ReyesPointReyesNo ratings yet
- Killing of Kangaroos For Meat and SkinDocument34 pagesKilling of Kangaroos For Meat and SkinVegan FutureNo ratings yet
- Principles of Inheritance and Variations: By: Dr. Anand ManiDocument113 pagesPrinciples of Inheritance and Variations: By: Dr. Anand ManiIndu YadavNo ratings yet
- Science of The Total Environment: Megan Carve Graeme Allinson, Dayanthi Nugegoda, Jeff ShimetaDocument16 pagesScience of The Total Environment: Megan Carve Graeme Allinson, Dayanthi Nugegoda, Jeff ShimetaFABIANA PASSAMANINo ratings yet
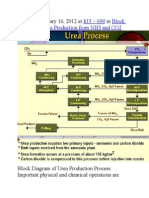
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Document9 pagesPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654No ratings yet
- Science Paper 7 - SolvedDocument10 pagesScience Paper 7 - SolvedRavi KumarNo ratings yet
- G.B.Pant University of Agriculture & Technology, Pantnagar-263145, Distt. Udham Singh Nagar (Uttarakhand) University Website: WWW - Gbpuat.ac - inDocument4 pagesG.B.Pant University of Agriculture & Technology, Pantnagar-263145, Distt. Udham Singh Nagar (Uttarakhand) University Website: WWW - Gbpuat.ac - inJeshiNo ratings yet
- Kami Export - Omarion Fladger - Pedigree Genetics ProblemsDocument2 pagesKami Export - Omarion Fladger - Pedigree Genetics ProblemsOmarion FladgerNo ratings yet
- 3 - Plasma Membrane and Transport MechanismsDocument67 pages3 - Plasma Membrane and Transport MechanismsThom PaglinawanNo ratings yet
- TGD FrameworkDocument10 pagesTGD FrameworkMatthew KleeNo ratings yet
- The Truth About Honey - White Paper PDFDocument5 pagesThe Truth About Honey - White Paper PDFSergio PérezNo ratings yet