You might also like
- Organizational Approaches To Improving Resuscitation EffectivenessDocument12 pagesOrganizational Approaches To Improving Resuscitation Effectivenessgiseladelarosa2006No ratings yet
- Uslam Bacterimeia Edad SexoDocument6 pagesUslam Bacterimeia Edad Sexogiseladelarosa2006No ratings yet
- Insulina SC UciDocument18 pagesInsulina SC Ucigiseladelarosa2006No ratings yet
- Jama Intern Med 2014 Aug 174 (8) 10 BenfitsDocument8 pagesJama Intern Med 2014 Aug 174 (8) 10 Benfitsgiseladelarosa2006No ratings yet
- Vasopresina Efectos AdversosDocument9 pagesVasopresina Efectos Adversosgiseladelarosa2006No ratings yet
- Cambios Resp Vena CavaDocument7 pagesCambios Resp Vena Cavagiseladelarosa2006No ratings yet
- HDFVVC EfectoDocument11 pagesHDFVVC Efectogiseladelarosa2006No ratings yet
- Visitas Policivas UciDocument4 pagesVisitas Policivas Ucigiseladelarosa2006No ratings yet
- Antioxidant EsDocument2 pagesAntioxidant Esgiseladelarosa2006No ratings yet
- Chest: Latent Class Analysis Identifi Es Distinct Phenotypes of Primary Graft Dysfunction After Lung TransplantationDocument7 pagesChest: Latent Class Analysis Identifi Es Distinct Phenotypes of Primary Graft Dysfunction After Lung Transplantationgiseladelarosa2006No ratings yet
- Clin Infect Dis. 2014 Lodise 666 75Document10 pagesClin Infect Dis. 2014 Lodise 666 75giseladelarosa2006No ratings yet
- Jama Intern Med 2014 Aug 174 (8) 2 MeaningDocument2 pagesJama Intern Med 2014 Aug 174 (8) 2 Meaninggiseladelarosa2006No ratings yet
- Jama Intern Med 2014 Aug 174 (8) 4 AntibioticDocument2 pagesJama Intern Med 2014 Aug 174 (8) 4 Antibioticgiseladelarosa2006No ratings yet
- JMN 140070Document2 pagesJMN 140070giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1106Document9 pagesIntensive Care Medicine 2014 40 (8) 1106giseladelarosa2006No ratings yet
- Jama Intern Med 2014 Aug 174 (8) 6 EvidenceDocument2 pagesJama Intern Med 2014 Aug 174 (8) 6 Evidencegiseladelarosa2006No ratings yet
- The Role of Copy-and-Paste in The Hospital Electronic Health RecordDocument2 pagesThe Role of Copy-and-Paste in The Hospital Electronic Health RecordHLMeditNo ratings yet
- Intensive Care Medicine 2014 40 (8) 1124Document8 pagesIntensive Care Medicine 2014 40 (8) 1124giseladelarosa2006No ratings yet
- Jama Intern Med 2014 Aug 174 (8) 2 MeaningDocument2 pagesJama Intern Med 2014 Aug 174 (8) 2 Meaninggiseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1151Document4 pagesIntensive Care Medicine 2014 40 (8) 1151giseladelarosa2006No ratings yet
- The Role of Copy-and-Paste in The Hospital Electronic Health RecordDocument2 pagesThe Role of Copy-and-Paste in The Hospital Electronic Health RecordHLMeditNo ratings yet
- Intensive Care Medicine 2014 40 (8) 1147Document4 pagesIntensive Care Medicine 2014 40 (8) 1147giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1115Document9 pagesIntensive Care Medicine 2014 40 (8) 1115giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1147Document4 pagesIntensive Care Medicine 2014 40 (8) 1147giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1106Document9 pagesIntensive Care Medicine 2014 40 (8) 1106giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1140Document4 pagesIntensive Care Medicine 2014 40 (8) 1140giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1097Document9 pagesIntensive Care Medicine 2014 40 (8) 1097giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1115Document9 pagesIntensive Care Medicine 2014 40 (8) 1115giseladelarosa2006No ratings yet
- Intensive Care Medicine 2014 40 (8) 1089Document8 pagesIntensive Care Medicine 2014 40 (8) 1089giseladelarosa2006No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Learning Stations Lesson PlanDocument3 pagesLearning Stations Lesson Planapi-310100553No ratings yet
- Individual Assignment ScribdDocument4 pagesIndividual Assignment ScribdDharna KachrooNo ratings yet
- SEO Design ExamplesDocument10 pagesSEO Design ExamplesAnonymous YDwBCtsNo ratings yet
- Numerical Methods: Jeffrey R. ChasnovDocument60 pagesNumerical Methods: Jeffrey R. Chasnov2120 sanika GaikwadNo ratings yet
- National Advisory Committee For AeronauticsDocument36 pagesNational Advisory Committee For AeronauticsSamuel ChristioNo ratings yet
- Unit 1 - Introduction To BankingDocument17 pagesUnit 1 - Introduction To Bankingc08No ratings yet
- sl2018 667 PDFDocument8 pagessl2018 667 PDFGaurav MaithilNo ratings yet
- ExpDocument425 pagesExpVinay KamatNo ratings yet
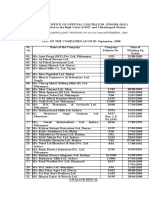
- Statement of Compulsory Winding Up As On 30 SEPTEMBER, 2008Document4 pagesStatement of Compulsory Winding Up As On 30 SEPTEMBER, 2008abchavhan20No ratings yet
- C Exam13Document4 pagesC Exam13gauravsoni1991No ratings yet
- Ijimekko To Nakimushi-Kun (The Bully and The Crybaby) MangaDocument1 pageIjimekko To Nakimushi-Kun (The Bully and The Crybaby) MangaNguyễn Thị Mai Khanh - MĐC - 11A22No ratings yet
- Singer NM37 57manualDocument266 pagesSinger NM37 57manualpaulkoby100% (2)
- 2016 Mustang WiringDocument9 pages2016 Mustang WiringRuben TeixeiraNo ratings yet
- DSE61xx Configuration Suite Software Manual PDFDocument60 pagesDSE61xx Configuration Suite Software Manual PDFluisNo ratings yet
- Conceptual FrameworkDocument24 pagesConceptual Frameworkmarons inigoNo ratings yet
- Report Daftar Penerima Kuota Telkomsel Dan Indosat 2021 FSEIDocument26 pagesReport Daftar Penerima Kuota Telkomsel Dan Indosat 2021 FSEIHafizh ZuhdaNo ratings yet
- NGPDU For BS SelectDocument14 pagesNGPDU For BS SelectMario RamosNo ratings yet
- Ground Water Resources of Chennai DistrictDocument29 pagesGround Water Resources of Chennai Districtgireesh NivethanNo ratings yet
- CL 5313 17021-1 Requirements Matrix-1458-5Document6 pagesCL 5313 17021-1 Requirements Matrix-1458-5Ana AnaNo ratings yet
- Inventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Document10 pagesInventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Wiro SablengNo ratings yet
- School Quality Improvement System PowerpointDocument95 pagesSchool Quality Improvement System PowerpointLong Beach PostNo ratings yet
- 5 Dec2021-AWS Command Line Interface - User GuideDocument215 pages5 Dec2021-AWS Command Line Interface - User GuideshikhaxohebkhanNo ratings yet
- 2019 May Chronicle AICFDocument27 pages2019 May Chronicle AICFRam KrishnaNo ratings yet
- Master of Commerce: 1 YearDocument8 pagesMaster of Commerce: 1 YearAston Rahul PintoNo ratings yet
- Planview Innovation Management Maturity Model PDFDocument1 pagePlanview Innovation Management Maturity Model PDFMiguel Alfonso Mercado GarcíaNo ratings yet
- Abinisio GDE HelpDocument221 pagesAbinisio GDE HelpvenkatesanmuraliNo ratings yet
- MSDS FluorouracilDocument3 pagesMSDS FluorouracilRita NascimentoNo ratings yet
- Active and Passive Voice of Future Continuous Tense - Passive Voice Tips-1Document5 pagesActive and Passive Voice of Future Continuous Tense - Passive Voice Tips-1Kamal deep singh SinghNo ratings yet
- CGV 18cs67 Lab ManualDocument45 pagesCGV 18cs67 Lab ManualNagamani DNo ratings yet
- WassiDocument12 pagesWassiwaseem0808No ratings yet