You might also like
- Flos CalendulaeDocument11 pagesFlos CalendulaeDestiny Vian DianNo ratings yet
- Flos Caryophylli: The Dried Flower Buds of Syzygium AromaticumDocument12 pagesFlos Caryophylli: The Dried Flower Buds of Syzygium AromaticumDestiny Vian DianNo ratings yet
- Radix GinsengDocument19 pagesRadix GinsengDestiny Vian DianNo ratings yet
- Herba CentellaeDocument10 pagesHerba CentellaeDestiny Vian DianNo ratings yet
- Skrining Fitokimia Herba AndrographidisDocument14 pagesSkrining Fitokimia Herba AndrographidisDewi YulaikahNo ratings yet
- Bulbus Allii SativiDocument19 pagesBulbus Allii SativiDestiny Vian DianNo ratings yet
- Radix ValerianaeDocument13 pagesRadix ValerianaeDestiny Vian DianNo ratings yet
- Radix GlycyrrhizaeDocument13 pagesRadix GlycyrrhizaeDestiny Vian DianNo ratings yet
- Rhizoma ZingiberisDocument12 pagesRhizoma ZingiberisDestiny Vian DianNo ratings yet
- Rhizoma Curcumae LongaeDocument12 pagesRhizoma Curcumae LongaeDestiny Vian DianNo ratings yet
- Bulbus Allii CepaeDocument12 pagesBulbus Allii CepaeDestiny Vian DianNo ratings yet
- Flos Caryophylli: The Dried Flower Buds of Syzygium AromaticumDocument12 pagesFlos Caryophylli: The Dried Flower Buds of Syzygium AromaticumDestiny Vian DianNo ratings yet
- Rhizoma RheiDocument11 pagesRhizoma RheiDestiny Vian DianNo ratings yet
- Flos CalendulaeDocument11 pagesFlos CalendulaeDestiny Vian DianNo ratings yet
- Radix RauwolfiaeDocument11 pagesRadix RauwolfiaeDestiny Vian DianNo ratings yet
- Cortex CinnamomiDocument11 pagesCortex CinnamomiDestiny Vian DianNo ratings yet
- Makalah Penelitian Tentang LingkunganDocument1 pageMakalah Penelitian Tentang LingkunganDedi IrhandiNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Herba ThymiDocument9 pagesHerba ThymiDestiny Vian DianNo ratings yet
- Folium EucalyptiDocument9 pagesFolium EucalyptiDestiny Vian DianNo ratings yet
- Folium Menthae PiperitaeDocument8 pagesFolium Menthae PiperitaeDestiny Vian DianNo ratings yet
- Fructus SennaeDocument10 pagesFructus SennaeDestiny Vian DianNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Monre BKMM 27 April 19 (Autosaved)Document14 pagesMonre BKMM 27 April 19 (Autosaved)AnggreanyAshariNo ratings yet
- Case Studies - NeurologyDocument12 pagesCase Studies - NeurologyNick MorettinNo ratings yet
- ERA System Brochure1Document6 pagesERA System Brochure1Ana Massiel NarváezNo ratings yet
- 1) KULLA, S. Lung Cancer Online VersionDocument83 pages1) KULLA, S. Lung Cancer Online VersionJosh SolisNo ratings yet
- NSVD Patient Sleep IssuesDocument3 pagesNSVD Patient Sleep IssuesAlma Gobaleza100% (1)
- Nursing Care Plan Cesarian DeliveryDocument2 pagesNursing Care Plan Cesarian Deliveryderic97% (39)
- Necessary Elements of A Dermatologic History and Physical Evaluation PDFDocument9 pagesNecessary Elements of A Dermatologic History and Physical Evaluation PDFkyle31No ratings yet
- CBG ProcedureDocument2 pagesCBG ProcedureMiden AlbanoNo ratings yet
- Guidelines HPNDocument46 pagesGuidelines HPNSherif AbobakrNo ratings yet
- Ncp-Ineffective Tissue Perfusion (Aortic Stenosis)Document2 pagesNcp-Ineffective Tissue Perfusion (Aortic Stenosis)Daniel Vergara Arce67% (3)
- Acute Intestinal ObstructionDocument3 pagesAcute Intestinal Obstructionoddone_outNo ratings yet
- Zimmer® Unicompartmental High Flex KneeDocument62 pagesZimmer® Unicompartmental High Flex Knee洪侊增No ratings yet
- Chapter 18 - PharmDocument35 pagesChapter 18 - PharmJames PerianayagamNo ratings yet
- Bio StatisticsDocument21 pagesBio StatisticsanaeshklNo ratings yet
- Pharmaceutical dosage capsules tabletsDocument6 pagesPharmaceutical dosage capsules tabletsLena EmataNo ratings yet
- Neonatal Energy Triangle Part 1Document6 pagesNeonatal Energy Triangle Part 1Belfast324100% (1)
- Case Scenario 2Document1 pageCase Scenario 2Sophia LaurieNo ratings yet
- Dip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017Document2 pagesDip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017matentenNo ratings yet
- Programme BroshureDocument2 pagesProgramme BroshureMagilas S. SalvacionNo ratings yet
- Multiple Associated Anomalies in Patients of Duodenal Atresia: A Case SeriesDocument2 pagesMultiple Associated Anomalies in Patients of Duodenal Atresia: A Case SeriesMuhammad Bilal MirzaNo ratings yet
- International Journal of Psychophysiology: Helen Beuzeron-Mangina, Constantine A. ManginaDocument6 pagesInternational Journal of Psychophysiology: Helen Beuzeron-Mangina, Constantine A. ManginaIcaroNo ratings yet
- Nexus Letter Providers - Updated 122022Document1 pageNexus Letter Providers - Updated 122022Jaster Da GreatNo ratings yet
- Figure FaultsDocument17 pagesFigure FaultsMichael SimpsonNo ratings yet
- Homeopathic Treatment of MigraineDocument3 pagesHomeopathic Treatment of MigraineRPh Krishna Chandra JagritNo ratings yet
- Chapter 12Document15 pagesChapter 12kk5522No ratings yet
- SLE Correct AnswersDocument20 pagesSLE Correct AnswersFiras AliNo ratings yet
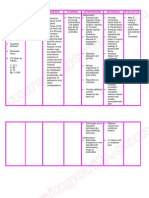
- III. Nursing Care Plan: Assessment Diagnosis Goal Intervention EvaluationDocument4 pagesIII. Nursing Care Plan: Assessment Diagnosis Goal Intervention EvaluationSTEPHANIE JOSUENo ratings yet
- SVT PresentationDocument39 pagesSVT PresentationReinsy NoviNo ratings yet
- Traumatic Brain Injury: Rehabilitation: Description of The Evidence Collection MethodDocument8 pagesTraumatic Brain Injury: Rehabilitation: Description of The Evidence Collection MethodDawud MuhammadNo ratings yet
- GlaukomaDocument41 pagesGlaukomadanufarandiNo ratings yet